




Abstract
Objectives
Wound complications are reported in up to 10% hip and knee arthroplasties and there is a proven association between wound complications and deep prosthetic infections. In this randomised controlled trial (RCT) we explore the potential benefits of a portable, single use, incisional negative pressure wound therapy dressing (iNPWTd) on wound exudate, length of stay (LOS), wound complications, dressing changes and cost-effectiveness following total hip and knee arthroplasties.
Methods
A total of 220 patients undergoing elective primary total hip and knee arthroplasties were recruited into in a non-blinded RCT. For the final analysis there were 102 patients in the study group and 107 in the control group.
Results
An improvement was seen in the study (iNPWTd) group compared to control in all areas. Peak post-surgical wound exudate was significantly reduced (p = 0.007). Overall LOS reduction (0.9 days, 95% confidence interval (CI) -0.2 to 2.5) was not significant (p = 0.07) but there was a significant reduction in patients with extreme values of LOS in the iNPWTd group (Moses test, p = 0.003). There was a significantly reduced number of dressing changes (mean difference 1.7, 95% CI 0.8 to 2.5, p = 0.002), and a trend to a significant four-fold reduction in reported post-operative surgical wound complications (8.4% control; 2.0% iNPWTd, p = 0.06).
Conclusions
Based on the results of this RCT incisional negative pressure wound therapy dressings have a beneficial role in patients undergoing primary hip and knee arthroplasty to achieve predictable length of stay, especially to eliminate excessive hospital stay, and minimise wound complications.
Cite this article: S. L. Karlakki, A. K. Hamad, C. Whittall, N. M. Graham, R. D. Banerjee, J. H. Kuiper. Incisional negative pressure wound therapy dressings (iNPWTd) in routine primary hip and knee arthroplasties: A randomised controlled trial. Bone Joint Res 2016;5:328–337. DOI: 10.1302/2046-3758.58.BJR-2016-0022.R1
Article focus
-
Wound complications in total hip and knee arthroplasty can lead to deep prosthetic infection, management of which can be difficult, expensive and with potential for disastrous outcomes.
-
Several factors such as wound healing, prolonged wound discharge, early discharge from hospital and management superficial wound complications influence the outcome.
-
Incisional negative pressure wound dressings may be a reasonable way of achieving improved predictability and safety in wound healing following hip and knee arthroplasty surgery.
Key messages
-
Incisional negative pressure wound therapy dressing appears to predictably improve wound discharge, wound healing, minimise wound complications and improve length of stay following routine hip and knee arthroplasties.
-
These dressings appear to be particularly beneficial in patients with an American Society of Anesthesiologists grade ⩾ 3 and a body mass index ⩾ 35 in reducing wound complications. The additional cost of these dressings is perhaps justifiable taking in to account all of these factors.
Strengths and limitations
-
This is a very first randomised controlled trial studying the effects of an innovative wound dressing using the beneficial aspects of negative pressure wound therapy in primary hip and knee arthoplasty, without compromising early post-operative mobilisation.
-
The limitations of this study being; this is a non-blinded study, the routine practice of changing wound dressings at the second day post-surgery and working towards expected date of discharge (four days post-surgery at the time of study period) was difficult to control, and the incidence of surgical wound complications were recorded rather than directly inspected.
Introduction
Total hip and knee arthroplasties (THA, TKA) are two of the most successful and predictable orthopaedic procedures. Although life changing,1 they can be associated with serious complications, sometimes with devastating consequences. Prolonged incisional wound drainage has been correlated with superficial surgical site and deep prosthetic infection.2-5 Incidence of post-operative wound complications is influenced by diabetes, obesity, quality of soft tissues, use of steroids, soft-tissue handling, and duration and complexity of surgery.6-8 Evidence is sparse regarding nutrition and wound healing.9 United Kingdom surgical site infection (SSI) surveillance data indicate that higher body mass index (BMI), longer duration of surgery and higher American Society of Anesthesiologists (ASA) grading increase the incidence of SSI in hip arthroplasties. For knee arthroplasties, on the other hand, it has been shown that female gender, as opposed to BMI, increases the incidence of SSI.10-12
With the changing economics in health care, length of stay (LOS) is increasingly seen as a preventable expense. Adoption of enhanced recovery protocols for hip and knee arthroplasties have reduced the LOS.9,13-16 However, early discharge from the hospital has the potential for wound complications being managed in the community and an increase in readmissions to hospital. This was recognised by the SSI reports and National Institute for Health and Care Excellence (NICE) publication on SSI arthroplasties.10,17 The economic and patient implications of superficial SSI leading to deep infection are well recognised.18-21 Therefore it is reasonable to argue that ‘predictable wound healing’ is a key factor in achieving overall ‘predictable outcome’.
The United Kingdom NICE, in a publication on surgical site infection,17 highlighted the gap in published evidence on the use of alternate wound dressings for incisional surgical wounds22-25 and suggested that chronic wound dressings could be used for surgical incisions to minimise the risk of SSI.
Negative pressure wound therapy (NPWT) is one such potential option. NPWT for chronic wounds was introduced in the early 90s;26,27 its effectiveness in chronic wounds, pressure sores and diabetic foot ulcers is well established.28-30 Over the last ten years the role of NPWT has been extended to acute wounds.31,32 Its application as a prophylactic measure for incisional wounds, although suggested as long ago as 2002 by Webb,33 remains a novel concept. In a recent review publication,34 the mechanisms of action of incisional NPWT have been attributed to improved blood supply,35-39 reduced lateral tension along wound edges,40-42 decrease in oedema,26,33,43-46 reduced subcutaneous haematoma and seroma,41,47,48 improved lymphatic drainage49 and prevention of wound contamination.43
The routine use of incisional NPWT until recently was largely restricted by the size of the apparatus and the expertise required in application of the dressing. However, with the introduction of smaller battery-operated, ultra-portable, single-use and disposable NPWT devices and ready-made incisional wound dressings,50,51 the concept of ‘incisional negative pressure wound therapy dressings’ (iNPWTd) has become more feasible. Currently there are two such devices marketed in the United Kingdom; one by Kinetic Concepts, Inc. (San Antonio, Texas) as Prevena, and the other by Smith & Nephew Healthcare Ltd (Hull, United Kingdom) as PICO. Both claim therapeutic effects equal to those of the larger traditional devices. PICO is a canister-less design with a sandwiched dressing component which allows negative pressure to be distributed across the skin and uses absorption and vaporisation to manage exudate from the wound (Fig. 1).52

Fig. 1
The negative pressure wound therapy dressing used in the study, PICO.
With the positive experiences of using these dressings in complex revision hip and knee surgery (publication awaiting), it was hypothesised that iNPWTd could be adopted for primary THAs and TKAs as a means of controlling wound exudate levels and therefore influencing the length of stay without increasing post discharge complications. A randomised controlled trial (RCT) was designed to evaluate iNPWTd effectiveness in patients undergoing primary elective hip and knee arthroplasties at our institution.
Patients and Methods
The objective of this study was to assess the potential benefits of the portable disposable incisional negative pressure wound therapy dressing in the setting of routine elective THAs and TKAs. The primary outcome was to measure the impact of iNPWTd on wound healing and effect on LOS. The secondary outcomes were assessment of wound complications such as prolonged wound exudate and superficial wound infections, number of dressing changes and the overall cost-effectiveness of the dressing.
The Smith & Nephew PICO dressing was chosen for the following reasons: the dressing is versatile with various size options, is smaller and has a quieter pump which is better tolerated by patients as shown by our clinical experience to date.
This was a non-blinded single-centre randomised controlled parallel group study in patients undergoing routine elective THAs and TKAs at our elective orthopaedic hospital. The study was designed and reported in line with the Consolidated Standards of Reporting Trials statement.53 The study was conducted between October 2012 and October 2013. The study period was from surgery to six week post-operative follow-up. Ethical approval was obtained from the National Research Ethics Service (NRES Committee South West – Exeter; REC No 12/SW/0094).
Three participating surgeons (SLK, NMG and RDB), experienced in performing primary and revision hip and knee joint arthroplasties took part in the study. All consecutive patients undergoing routine THAs and TKAs (for any indication) under these three consultant surgeons were approached by the surgeon or his registrar, and willing patients were recruited to the study, provided they met the study inclusion and exclusion criteria. Patients who had known allergies to dressings, were undergoing revision joint surgery, were unwilling to attend additional clinics, and those on warfarin were excluded. Patients on warfarin were excluded primarily because of the anticipated extended LOS to allow their prothrombin time and international normalised ratio (INR) to reach therapeutic levels before being discharged.
Patient consent and randomisation were undertaken by the research team upon admission. The randomisation was performed using sealed opaque envelopes with a block size of 20 shuffled envelopes with a 1:1 allocation. These envelopes were prepared in advance and were opened by the research personnel for the recruited patient on the day of surgery. The first patient was enrolled into the study on 5 October 2012. A total of 220 patients were recruited into the trial, with 110 in each group.
The dressings were applied in theatre immediately after the wound closure. The study group received PICO NPWT dressings and the control group received conventional dressings: either Mepore (Mölnlycke Health Care AB, Gothenburg, Sweden) or Tegaderm (3M Health Care Ltd, Loughborough, United Kingdom) as per the surgeon’s preferred practice. All patients received 1.5 g of cefuroxime antibiotic at induction and one dose post-surgery. Patients were operated on by either the consultant surgeon or by the trainee under direct supervision. Wounds were closed in a layered fashion with skin staples or subcuticular Monocryl (Ethicon Inc., Johnson-Johnson, New Brunswick, New Jersey) sutures to close the skin.
For the NPWT group the protocol was to leave the dressing in place for a week (design of PICO and pump is programmed to last seven days). The control group patients had their dressing changed to OPSITE Post-Op Visible dressing (Smith & Nephew Healthcare Ltd) on the second post-operative day as per the usual routine practice. For both groups the dressing was changed earlier or again if there was progressive exudate filling 50% or more of the dressing. All patients received enoxaparin (clexane; Sanofi-Aventis, Holmes Chapel, United Kingdom) post-surgery (four weeks for hips and two weeks for knees). In the hospital, patients were seen on a daily basis in the morning by the same team of two research personnel, in order to minimise errors and maintain consistency. The following information was recorded: level of wound exudate, any dressing change and reasons, discharge readiness from a wound perspective, LOS and reasons for delay in discharge.
Wound exudate level was graded on a five-point scale based on the fraction of the wound length stained by exudate as noted on the dressing (Table I). The length of the dressing was split into four quarters for this measurement. Where there was minimal staining along the length of the incision wound, this was assessed as either grade 1 or 2 based on lateral spread. No standardised-validated methodology exists for this assessment, but given the essentially one-dimensional nature of the wound, this methodology was deemed reasonable for the study. If the dressing was changed prior to morning inspection, the extent of exudate at the time of dressing change was captured as a part of data collection, as was the reason for changing the dressing.
Table I.
Grading of wound exudate levels
| Grade | Amount of exudate | Coverage of dressing |
|---|---|---|
| Grade 0 | None | No staining |
| Grade 1 | Light | < 25% |
| Grade 2 | Moderate | 25% to 50% |
| Grade 3 | Heavy | 50% to 75% |
| Grade 4 | Overt | > 75% |
From the wound perspective, the patient discharge criteria were set at dry dressing or non-progressive minimal staining on the dressing. All patients were subjected to an enhanced recovery protocol following surgery, and discharged home when medically safe and sufficient home/community care was in place.
Post-discharge, all patients were contacted by telephone at two weeks post-surgery, and in addition the study group were seen in a wound clinic (by the same wound care nurse) at one week post-surgery to ensure safety with the new dressing and removal of the iNPWTd. All patients were seen at six weeks post-surgery in the consultant-led follow-up clinic as per routine practice. Wound-related complications such as recurrence of wound exudate, surgical site infections, dressing-related issues, readmission to hospital and any further surgical interventions were documented at each encounter by the research personnel.
Statistical analysis
The exudate level measurements were summarised as a single variable by their peak level. Distributions of all variables were investigated for normality using Quantile-Quantile (Q-Q) plots, which plot the quantiles of a variable against the quantiles of a normal distribution with the same mean and standard deviation. Analysis of LOS was based on the intention to treat (ITT) population, whereas analyses of wound properties were based on the per protocol (PP) population because those outcomes were only collected for this population. Subanalysis based on stratification by hip or knee surgery was performed. Mean LOS of the two groups was analysed using a non-parametric method specifically developed for highly skewed data (method T3).54 Differences in peak wound exudate level and complication rates were analysed using Fisher’s exact test. The influence of confounding factors was analysed using a logistic regression model or a proportional odds logistic model. Conditional inference trees and model-based recursive partitioning were used to find meaningful treatment-subgroup interactions. The sample size was chosen to permit detection of a difference in LOS of 0.6 days, assuming a two-tailed significance level of p = 0.05 and 80% power, and based on a standard deviation of 1.5 days as found in an earlier study at our institution.55 All statistical analyses were performed using R v 3.0.3 (R Foundation for Statistical Software, Vienna, Austria) and G*Power v 3.1.3 (University of Düsseldorf, Germany). A two-tailed p-value below 0.05 was assumed to denote statistical significance.
Results
The ITT population consisted of 108 patients in the control group (two patients in the control group had their surgery cancelled on the day) and 107 patients in the study group (two patients in the study group withdrew consent after randomisation and a third immediately after surgery) (Fig. 2).
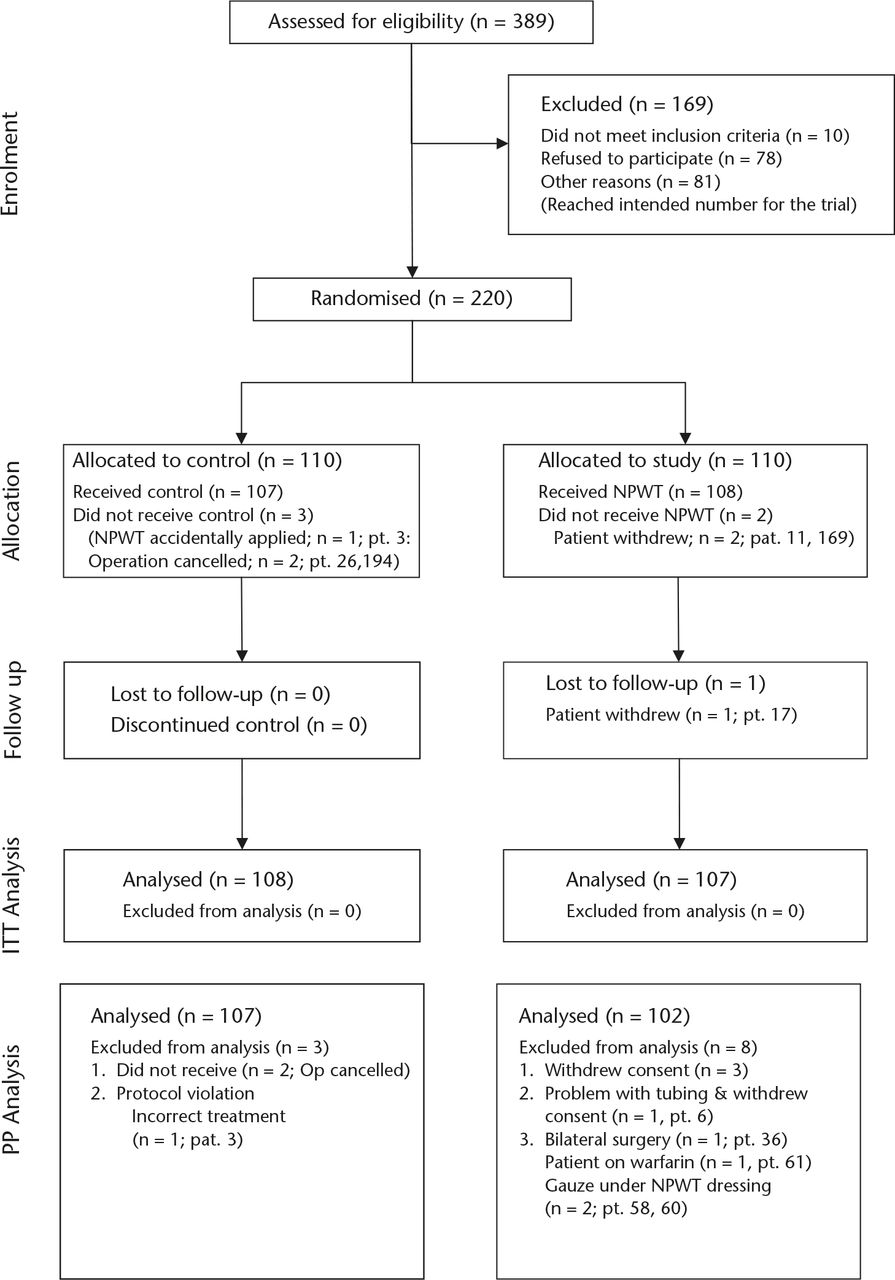
Fig. 2
Consolidated Standards of Reporting Trials diagram for negative pressure wound therapy (NPWT) dressings.
The PP population consisted of 107 patients in the control group (one further patient received NPWT dressing by error) and 102 in the study group (one further patient withdrew two days post-operatively due to problems with the tubing on dressing, and four further patients due to protocol deviations as shown in Fig. 2).
Demographics
Based on the PP population of 209 patients, there were 116 hip arthroplasties and 93 knee arthroplasties. The patient demographics are shown in Table II. The two groups were well balanced, except for the fact that the proportion of patients with a BMI > 35 in the study group (17%) was twice that in the control group (8%). On average, the patients had two of the following comorbidities: BMI > 30 (82), hypertension (76), hypercholesterolaemia (32) and diabetes (17).
Table II.
Distribution of patients between two groups
| Study n (%) | Control n (%) | |
|---|---|---|
| Patients | 102 | 107 |
| Female | 53 (52) | 52 (49) |
| Male | 49 (48) | 55 (51) |
| Age (yrs, mean (sd)) | 69.0 (9.0) | 69.2 (9.0) |
| Joint replaced (n, %) | ||
| Hip | 53 (52) | 63 (59) |
| Knee | 49 (48) | 44 (41) |
| BMI (mean (sd)) | 30.1 (5.0) | 28.4 (4.6) |
| ASA score | ||
| 1 | 23 (24) | 24 (23) |
| 2 | 60 (64) | 69 (66) |
| 3 | 11 (12) | 11 (11) |
| Comorbidities (n, %) | ||
| Number of comorbidities (mean, sd) | 1.9 (1.5) | 1.7 (1.5) |
| Any | 80 (78) | 80 (75) |
| Obesity (body mass index ⩾ 35) | 17 (17) | 9 (8) |
| Morbid obesity (body mass index ⩾ 40) | 3 (3) | 1 (1) |
| Smoking (current or previous) | 14 (22) | 13 (22) |
| Diabetes | 5 (5) | 12 (11) |
| Anaesthetic (n, %) | ||
| GA & SA | 46 (45) | 49 (46) |
| SA | 33 (32) | 31 (29) |
| SA & Sedation | 14 (14) | 15 (14) |
| GA | 7 (7) | 9 (8) |
| Other (n = 1 or n = 2 each) | 2 (2) | 3 (3) |
| Drain usage (n, %) | ||
| Yes | 50 (49) | 47 (44) |
| H-27, K-23 | H-26, K-21 | |
| No | 52 (51) | 60 (56) |
| Wound closure (n, %) | ||
| Staples | 76 (75) | 73 (68) |
| H-35, K-41 | H-44, K-29 | |
| Sutures | 26 (25) | 34 (32) |
| H-18, K-8 | H-19, K-15 | |
| Surgeon (%) | ||
| 1 (Mr Karlakki) | 49 | 42 |
| K-23, H-27 | K-21, H-24 | |
| 2 (Mr Graham) | 31 | 38 |
| K-16, H-16 | K-20, H-21 | |
| 3 (Mr Banerjee) | 20 | 20 |
| K-10, H 10 | K-3, H-18 |
-
H, hip; K, knee; sd, standard deviation; GA, general anaesthetic; SA, spinal anaesthetic
Wound exudate
The majority of patients, as anticipated in a routine primary joint arthroplasty, had grade 0 to 2 peak level of exudate (Fig. 3, Table III). The level and number of peak exudates differed significantly between the two groups (Fisher’s exact test, p = 0.007), with more patients in lower grades and fewer patients in higher grades in the study group compared with the control group. Only 4% of the study group had grade 4 exudate as compared with 16% in the control group, a four-fold reduction. The number of patients who had grade 3 exudate was small in both groups. The difference in peak exudate level between the two groups did not depend significantly on the procedure (hip versus knee, multinomial regression, interaction term p = 0.38).
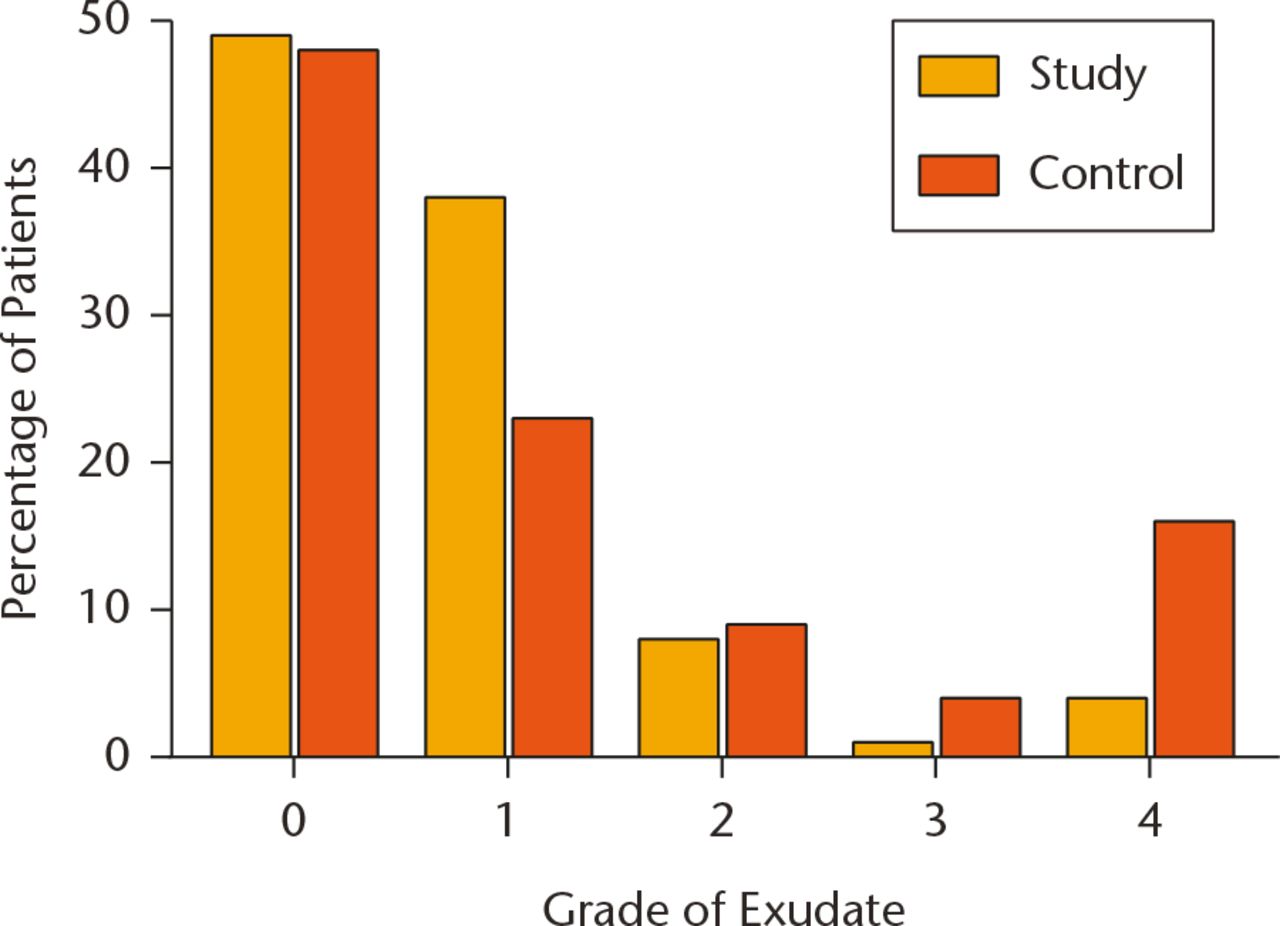
Fig. 3
Distribution of peak exudate levels between the two study groups.
Table III.
Distribution of peak exudate levels between the two study groups and between hip and knee arthroplasty (n, %)
| Grade | All patients |
Hip patients |
Knee patients |
|||
|---|---|---|---|---|---|---|
| Study | Control | Study | Control | Study | Control | |
| 0 | 50 (49) | 51 (48) | 26 (49) | 34 (54) | 24 (49) | 17 (39) |
| 1 | 39 (38) | 25 (23) | 24 (45) | 15 (24) | 15 (31) | 10 (23) |
| 2 | 8 (8) | 10 (9) | 1 (2) | 4 (6) | 7 (14) | 6 (14) |
| 3 | 1 (1) | 4 (4) | 0 (0) | 3 (5) | 1 (2) | 1 (2) |
| 4 | 4 (4) | 17 (16) | 2 (4) | 7 (11) | 2 (4) | 10 (23) |
-
Differences significant for all patients (p = 0.007) and hip patients (p = 0.04) but not for knee patients (p = 0.09), all Fisher’s exact test.
Two confounding factors, use of drain and skin closure with staples, influenced wound exudate levels following surgery. Drains reduced peak exudate by a factor of 5 (grades 3 and 4), and staples reduced the overall exudate levels, but not grade 4. The usage of drains and skin staples between the two groups was similar (Table II).
Length of stay
Over 50% of the patients were discharged within three days of their surgery in both groups. The range and spread of LOS was smaller for the study group (one to ten days) as compared with the control group (two to 61 days) (Table IV). Extreme values for LOS were significantly lower in the study group (Moses test, p = 0.003).
Table IV.
Distribution of length of stay (LOS) between two groups, per protocol analysis
| Length of stay(days) | Study | Control |
|---|---|---|
| 1 | 1 | 0 |
| 2 | 28 | 20 |
| 3 | 28 | 36 |
| 4 | 16 | 19 |
| 5 | 13 | 15 |
| 6 | 7 | 3 |
| 7 | 2 | 5 |
| 8 | 3 | 4 |
| 9 | 3 | 1 |
| 10 | 1 | 0 |
| 11 | 0 | 1 |
| 12 | 0 | 0 |
| 13 | 0 | 1 |
| 27 | 0 | 1 |
| 61 | 0 | 1 |
-
Extreme values of LOS were significantly lower in the study group (Moses test, p = 0.003)
The mean LOS for the ITT population was 3.8 days (95% (confidence interval) CI 3.5 to 4.2) for the study group and 4.7 days (95% CI 3.8 to 6.4) for the control group (difference 0.9 days, 95% CI -0.2 to 2.5, p = 0.07). This reduction in LOS, although measurable, was not statistically significant (Table V). The LOS was not markedly different for the PP population. The study group had a significantly smaller probability of excess LOS due to wound leakage (odds ratio (OR) 0.11, 95% CI 0.002 to 0.81, p = 0.02).
Table V.
Mean and median length of stay (LOS) estimates for the two groups
| Mean (95% CI) | Median (IQR) | Range | p-value | |
|---|---|---|---|---|
| Total LOS (days)* | ||||
| Study | 3.8 (3.5 to 4.2) | 3 (2 to 5) | 1 to 10 | |
| Control | 4.7 (3.8 to 6.4) | 3 (3 to 5) | 2 to 61 | |
| Difference | 0.9 (-0.2 to 2.5) | 0.07 | ||
| Total LOS (days)† | ||||
| Study | 3.8 (3.5 to 4.3) | 3 (2 to 5) | 1 to 10 | |
| Control | 4.7 (3.8 to 6.4) | 3 (3 to 5) | 2 to 61 | |
| Difference | 0.9 (-0.1 to 2.5) | 0.09 | ||
| Total capped LOS (days)† | ||||
| Study | 3.8 (3.5 to 4.3) | 3 (2 to 5) | 1 to 10 | |
| Control | 4.1 (3.8 to 4.7) | 3 (3 to 5) | 2 to 13 | |
| Difference | 0.3 (-0.2 to 1.0) | 0.19 |
-
All 95% confidence intervals (CI) and p-values for difference calculated using Zhou and Dinh’s method T3
-
*
Analysis based on Intention To Treat population
-
†
Analysis based on Per Protocol population
-
IQR, interquartile range
The mean LOS for the control group was strongly affected by two outliers, both related to wound complications. To analyse the sensitivity to these two outliers, their LOS was capped at 13 days (the third shortest LOS in the control group). This reduced the LOS of the control group to 4.1 days (95% CI 3.8 to 4.7) and the difference in LOS to 0.3 days (95% CI -0.16 to 1.0), still shorter for the study group (Table V). The LOS was significantly affected by several confounding factors such as age, ASA grade and drain usage, but also by factors more difficult to quantify such as a ward culture of working towards expected date of discharge and social factors delaying discharge. The influence of these confounding factors across the two groups was not significant.
Wound complications
A total of 11 out of 209 (5.2%) patients encountered surgical wound-related complications (Table VI) and nine of these were following discharge from the hospital. Wound complications were mainly in the control group and in knee arthroplasties. Therefore, the majority of these complications (9/11) were recorded (two-week phone call check) rather than directly inspected.
Table VI.
Wound complications noted post-operatively (up to 6 weeks follow-up) for the two groups
| Group | BMI/ Gender | Surgery | ASA grade | Comorbidities | Post-operative complication |
|---|---|---|---|---|---|
| Control* | 44.96 / M | TKA | 3 | HTN, DM Type II, BMI > 35 | Haematoma, SSSI, delayed wound healing |
| Control | 37.56 / F | TKA | 2 | BMI > 35 | Superficial wound infection |
| Control | 24.82 / M | TKA | 3 | None | Superficial wound infection |
| Control | 24.74 / F | TKA | 2 | None | Superficial wound infection |
| Control | 29.09 / F | THA | 2 | HTN, High cholesterol, Previous chemotherapy | Prolonged wound discharge and healing |
| Control | 29.08 / F | TKA | 2 | Osteoporosis, Previous chemotherapy and radiotherapy, Lymphoma | Prolonged wound discharge and healing |
| Control | 27.04 / M | TKA | 3 | HTN, CKD stage 3, CVA, Polymyalgia Rheumatica, Ex-smoker | Superficial wound infection |
| Control | 34.58 / F | THA | 3 | Smoker, Borderline DM, HTN, Asthma | Superficial wound infection |
| Control* | 29.39 / M | THA | 2 | DM Type II, HTN, High cholesterol, Ex-smoker | Prolonged wound discharge |
| Study | 44.09 / F | TKA | 3 | BMI >35, Lymphoedema, Cellulitis, Eczema | Prolonged wound discharge and healing, SSSI |
| Study | 40.09 / M | TKA | 2 | BMI > 35 | Prolonged wound discharge/cellulitis |
-
All wounds with complications were closed with staples
-
*
complications arose during in-patient stay, all other complications were treated in the community (either by GP or District Nurse). Post-operative wound-related complications for the two groups, difference significant (p = 0.06; Fisher’s exact test) with an OR (95%) 4.0 (0.95 to 30)
-
BMI, body mass index; TKA, total knee arthroplasty; THA, total hip arthroplasty; ASA, American Society of Anesthesiologists; HTN, hypertension; DM, diabetes mellitus; CKD, chronic kidney disease; CVA, stroke; SSSI, skin and skin structure infection
In the control group, nine patients (8.4%) developed wound complications following surgery: two as inpatients (one following knee and one following hip arthroplasty; both had prolonged wound exudate and required surgical washouts) and seven following discharge from the hospital. The complications were exudating wounds and the majority (7/9) were treated for suspected superficial SSI with antibiotics in the community. One other patient was re-admitted for pain and stiffness following knee arthroplasty and underwent arthroscopic washout.
In the study group, two patients (2.0%) developed wound complications following discharge. Both were morbidly obese (BMI > 40) and had knee arthroplasties; one had been treated with antibiotics by their general practitioner for cellulitis. There were no late consequences in either group.
Overall there was a four-fold reduction in post-operative wound complications (OR 4.0, 95% CI 0.95 to 30, p = 0.06 Fisher’s exact test) in the study group compared with the control group. This difference in incidence of wound complications - study group 2% and control group 8.4% - was just below statistically significant. Recursive-partitioning analysis suggested that iNPWTd would be beneficial specifically for patients with an ASA grade ⩾ 3 and a BMI ⩾ 35 (p = 0.02 for iNPWTd × group-membership interaction term). A higher BMI, ASA grade, diabetes, smoking/former smoking and skin closure with staples were factors that increased the risk of wound complications across the two groups (Table VII) and the spread of these factors was similar across the two groups (Table II).
Table VII.
Influence of confounding factors on wound complications
| Confounding factors | OR (95% CI) | p-value |
|---|---|---|
| ASA | – | 0.003* |
| Body mass index (BMI) | 1.2 (1.04 to 1.3) | 0.007† |
| Obesity (BMI ⩾ 35) | 4.5 (1.1 to 16) | 0.03* |
| Morbid obesity (BMI ⩾ 40) | 68 (6.7 to 1904) | < 0.001* |
| Diabetes | 4.9 (1.0 to 20) | 0.05* |
| Smoking | – | 0.006* |
| Procedure (TKA vs THA) | 3.5 (0.84 to 16) | 0.07* |
| Anaesthetic | – | 0.05* |
| Wound closure method (suture vs staple) | 0.0 (0.0 to 0.90) | 0.04* |
-
*
p-value based on Fisher’s exact test
-
†
p-value based on logistic regression model
-
OR, odds ratio; CI, confidence intervals; ASA, American Society of Anesthesiologists; TKA, total knee arthroplasty; THA, total hip arthroplasty
The other notable complication was an occurrence of blisters in the study group (11%) and the control group (1%). Blisters were minor (< 1cm) and seen around the composite/adhesive junction of the dressing, about 2 cm from the incision and mainly in knee arthroplasties (18%, THA - 3.7%). Blisters were inspected in the study group (at one-week wound check) and noted for the control group at two weeks phone call check. All patients healed without further complications. There was a wide variation in the occurrence of blisters in the study group between three surgeons (surgeon 1: 4% (one TKA, one THA), surgeon 2: 21.2% (six TKA, one THA) and surgeon 3: 10.5% (two TKA) and highest for a surgeon who relied on the trainee to apply the dressing). Avoiding stretching of the dressing and applying to a flexed knee appeared to minimise blisters once this was recognised.
Dressing changes
In the study group, the intention was to leave on the iNPWT dressing, which was designed to be left untouched for a week unless the amount of exudate dictated otherwise (exudate filling more than 50% of the dressing). For the control group, as per the routine, there would be a minimum of one dressing change and further changes based on the extent and amount of wound exudate (exudate filling more than 50% of the dressing). There was a significant reduction in the mean number of dressing changes in the study group (2.5 95% CI 2.2 to 2.8) compared with the control group (4.2 95% CI 3.6 to 5.2) (p = 0.002; difference 1.7 95% CI 0.8 to 2.5). The dressing changes in the study group were due to a combination of factors: five were due to excessive wound exudate, others were device-related and a further unintended few were as a result of routine practice in the ward.
Cost effectiveness
There is a cost factor associated with iNPWTd; PICO seven-day treatment systems are marketed at £125, substantially more expensive than the traditional wound dressing. Taking into account reduced LOS for the study group (£275 per day hospital bed),56 fewer wound complications, fewer dressing changes (nurse time) and potential cost savings for wound care in the community due to reduced number of wound complications in the study group, the additional cost of the iNPWTd appears justifiable; however, we accept that a detailed analysis of financial modelling is required and a more detailed analysis will be the subject of a future publication.
Overall, the iNPWTd was easy to apply and well tolerated by patients. There were a few device-related issues: one pump failure and ten suction tube disconnections from dressing or the pump due to the long tube getting in the way whilst changing clothes and mobilising. Eight additional patients required re-application of the iNPWTd as a result of loss of vacuum, unrelated to the dressing. The PICO NPWT system is supplied with one pump and two separately packed dressings. The second dressing was used in 25% of patients.
Discussion
During 2013 and 2014, nearly 200 000 hip and knee arthroplasties were performed in the United Kingdom and the proportion of patients with higher ASA and BMI undergoing hip and knee arthroplasty has increased over the years.57 Post-discharge wound complication rates reported by patients via PROMS (patient-reported outcome measures) are much higher (10% of hip arthroplasties and 13% of knee arthroplasties)57 than those recognised by SSI reports.11,12 Considering both data do not represent the whole population, the realistic SSI is probably somewhere in between.
Management of wound complications in the community can be variable. Eventual complications such as deep prosthetic infection requiring revision surgery are not only devastating to the patient, but are also a negative performance indicator for the treating surgeon. National joint registries in most countries now collect this information against the surgeon. Therefore it is not surprising that surgeons prefer to keep patients in hospital until the wound is dry to minimise post-discharge complications, which can be a limiting factor for a timely discharge from hospital. Consequently it is reasonable to argue that there is a need for a predictable way of managing surgical wounds following joint arthroplasties, and portable iNPWTd may be a way of achieving this.
In this first RCT studying the effects of iNPWTd on wound healing in primary hip and knee arthroplasties, we found improvements in all of the areas we set out to assess. Wound exudates were significantly lower in the study group (p = 0.007). This was particularly the case for grade-4 exudate, where there was a four-fold reduction for the study group. There was a reduction in LOS for the study group (0.9 days, 95% CI -0.1 to 2.5, p = 0.07). Although this reduction was influenced by the two outlier patients, both patients had in fact remained longer in hospital for wound-related complications and subsequent treatment. Even when capped at 13 days the difference in LOS was still shorter for the study group patients. Further analysis also indicates that the extreme values for LOS are significantly improved by iNPWTd (Moses test, p = 0.003), suggesting a better predictability in LOS with iNPWTd. There was a four-fold reduction in post-operative wound-related complications (OR 4.0, 95% CI 0.95 to 30), although this did not reach statistical significance (p = 0.06). Two of the patients in the control group had persistent wound exudate and required formal surgical washouts resulting in excessive LOS; this was not seen in the study group. Accepting that the complications noted in the community were recorded rather than inspected complications, these were again mainly in the control group, indicating better wound healing with iNPWTd. Our analyses also suggested that iNPWTd would be beneficial specifically for patients with an ASA ⩾ 3 and a BMI ⩾ 35 in reducing wound complications. As expected, there was a reduction in requirement for dressing changes (p = 0.002).The cost of iNPWTd is perhaps justifiable if one were to take into account the additional cost incurred due to increased wound complications, increased dressing changes and resultant increase in LOS in the control group.
There are a number of limitations to this study: a) this was a non-blinded study, given the obvious difference between the two dressings, both to research personnel as well as to the clinician; b) the routine practice of changing wound dressings at second day post-surgery and working towards expected date of discharge (four days post-surgery at the time of study period) was difficult to control, due to the number of nursing staff involved in patient care; c) the incidence of surgical wound complications was recorded rather than directly inspected as the information was obtained over telephone at the two-week telephone check; d) wound-related data were not collected following protocol failure, which meant an ITT analysis was only possible for LOS; and finally, e) we were unable to standardise the wound closure methodology, as this would have meant changing surgeons’ practice.
Skin staples have been implicated in the increased risk of wound complications.58,59 An RCT looking at this specifically in hip and knee arthroplasties reports otherwise.60 In this study, wound closure with skin staples was a confounding factor for wound complications, as was knee arthroplasty as opposed to hip arthroplasty, ASA ⩾ 3 and BMI ⩾ 35 (Table VII). On the other hand, interestingly, wound complications were far lower in the study group despite the higher usage of skin staples as compared with the control group (Table II). Two patients in the study group who had wound complications had a BMI of > 40 and had knee arthroplasties. The choice for skin staples for surgeons with mixed practice was influenced by the quality of the skin (poor or thin skin not amenable to subcuticular suture). Additionally, there were twice as many patients with BMI ⩾ 35 in the study group. Therefore, iNPWTd appears to reduce the risk of wound complication and enhance wound healing despite these confounding factors; this, we feel, is a result of reduction in wound oedema and stabilisation of wound edges.
As with any new device there are a few clinical and practical issues. The long tubing is prone to detachment and the pump lacks an integral clip for attachment to clothing (which resulted in one patient withdrawing from the study). This dressing is not suitable when there is excessive wound ooze and considerations must be given for a surgical washout. Blisters, as reported previously,61 are an issue with iNPWTd. These are minor, away from wound edges and minimised with careful application of the dressing.
In conclusion, based on the study findings, iNPWTd offers a safe and predictable control of wound exudate in incisional wounds following hip and knee arthroplasties. It could allow patients to be discharged early without an exudating wound or post-discharge wound complications being a limiting factor. Incisional iNPWTd may be a choice where there is a rapid turnover of patients and bed planning is crucial. Perhaps for these dressings to be truly versatile and further conducive to their use in hip and knee arthroplasty, the pump needs to be smaller and form an integral part of the dressing.
We thank the Research team at RJAH for all their hard work and Smith & Nephew Scientific & Medical affairs, Dr R. Martin and Dr V. Strugala for helpful discussions.
Funding Statement
The study was funded through a grant from Smith & Nephew UK, to cover the cost of NPWT dressings and data collection costs.
S. Karlakki declares that he has received payment and funding for consultancy work, lectures and other projects unrelated to this paper.
C. Whitall declares she has received payment from Smith & Nephew for other work unrelated to this paper.
ICMJE conflict of interest
None declared.
References
1 Norman-Taylor FH , PalmerCR, VillarRN. Quality-of-life improvement compared after hip and knee replacement. J Bone Joint Surg [Br]1996;78-B:74-77.PubMed Google Scholar
2 Patel VP , WalshM, SehgalB, et al.. Factors associated with prolonged wound drainage after primary total hip and knee arthroplasty. J Bone Joint Surg [Am]2007;89-A:33-38.CrossrefPubMed Google Scholar
3 Weiss AP , KrackowKA. Persistent wound drainage after primary total knee arthroplasty. J Arthroplasty1993;8:285-289.CrossrefPubMed Google Scholar
4 Abudu A , SivardeenKA, GrimerRJ, PynsentPB, NoyM. The outcome of perioperative wound infection after total hip and knee arthroplasty. Int Orthop2002;26:40-43.CrossrefPubMed Google Scholar
5 Saleh K , OlsonM, ResigS, et al.. Predictors of wound infection in hip and knee joint replacement: results from a 20 year surveillance program. J Orthop Res2002;20:506-515.CrossrefPubMed Google Scholar
6 Peel TN , DowseyMM, DaffyJR, et al.. Risk factors for prosthetic hip and knee infections according to arthroplasty site. J Hosp Infect2011;79:129-133.CrossrefPubMed Google Scholar
7 Jones RE , RussellRD, HuoMH. Wound healing in total joint replacement. Bone Joint J2013;95-B:144-147.CrossrefPubMed Google Scholar
8 Ridgeway S , WilsonJ, CharletA, et al.. Infection of the surgical site after arthroplasty of the hip. J Bone Joint Surg [Br]2005;87-B:844-850.CrossrefPubMed Google Scholar
9 Ibrahim MS , KhanMA, NizamI, HaddadFS. Peri-operative interventions producing better functional outcomes and enhanced recovery following total hip and knee arthroplasty: an evidence-based review. BMC Med2013;11:37.CrossrefPubMed Google Scholar
10 Elgohari S , MihalkovaM, WlochC, et al.. Health Protection Agency. Surveillance of Surgical Site Infections in NHS Hospitals in England, 2013/14. https://www.gov.uk/government/uploads/system/uploads/attachment_data/file/386927/SSI_report_2013_14_final__3_.pdf (date last accessed 23 May 2016). Google Scholar
11 Elgohari S , MihalkovaM, HarringtonP, et al.. Health Protection Agency. Surveillance of Surgical Site Infections in NHS Hospitals in England, 2012/2013. https://www.gov.uk/government/uploads/system/uploads/attachment_data/file/364319/SSI_annual_report_2012_to_13_final.pdf (date last accessed 23 May 2016). Google Scholar
12 Elgohari S , MihalkovaM, WlochC, et al.. Surveillance of Surgical Site Infections in NHS Hospitals in England, 2013/2014. https://www.gov.uk/government/uploads/system/uploads/attachment_data/file/386927/SSI_report_2013_14_final__3_.pdf (date last accessed 20 May 2016). Google Scholar
13 Malviya A , MartinK, HarperI, et al.. Enhanced recovery program for hip and knee replacement reduces death rate. Acta Orthop2011;82:577-581.CrossrefPubMed Google Scholar
14 Marques EM , JonesHE, ElversKT, et al.. Local anaesthetic infiltration for peri-operative pain control in total hip and knee replacement: systematic review and meta-analyses of short- and long-term effectiveness. BMC Musculoskelet Disord2014;15:220.CrossrefPubMed Google Scholar
15 Starks I , WainwrightTW, LewisJ, LloydJ, MiddletonRG. Older patients have the most to gain from orthopaedic enhanced recovery programmes. Age Ageing2014;43:642-648.CrossrefPubMed Google Scholar
16 Jørgensen CC , KehletH, Lundbeck Foundation Centre for Fast-track Hip and Knee Replacement Collaborative Group. Role of patient characteristics for fast-track hip and knee arthroplasty. Br J Anaesth2013;110:972-980.CrossrefPubMed Google Scholar
17 No authors listed. NICE National Institute for Clinical Excellence, Surgical site infection: Prevention and treatment of surgical site infection. https://www.nice.org.uk/guidance/cg74/evidence/full-guideline-242005933 (date last accessed 23 May 2016). Google Scholar
18 Jenks PJ , LaurentM, McQuarryS, WatkinsR. Clinical and economic burden of surgical site infection (SSI) and predicted financial consequences of elimination of SSI from an English hospital. J Hosp Infect2014;86:24-33.CrossrefPubMed Google Scholar
19 de Lissovoy G , FraemanK, HutchinsV, et al.. Surgical site infection: incidence and impact on hospital utilization and treatment costs. Am J Infect Control2009;37:387-397.CrossrefPubMed Google Scholar
20 Doherty GM . Post-operative complications. In: DohertyGM, WayLW, eds. Current Surgical Diagnosis & Treatment. Twelfth ed. New York: Lange Medical Books/McGraw-Hill, 2006:21.CrossrefPubMed Google Scholar
21 National Nosocomial Infections Surveillance System. National Nosocomial Infections Surveillance (NNIS) System Report. Data summary from January 1992 through June 2004, issued October 2004. Am J Infect Control2004;32:470-485. Google Scholar
22 Tustanowski J . Effect of dressing choice on outcomes after hip and knee arthroplasty: a literature review. J Wound Care2009;18:449-450, 452, 454, passim.CrossrefPubMed Google Scholar
23 Walter CJ , DumvilleJC, SharpCA, PageT. Systematic review and meta-analysis of wound dressings in the prevention of surgical-site infections in surgical wounds healing by primary intention. Br J Surg2012;99:1185-1194.CrossrefPubMed Google Scholar
24 Dumville JC , WalterCJ, SharpCA, PageT. Dressings for the prevention of surgical site infection. Cochrane Database Syst Rev2011;CD003091.CrossrefPubMed Google Scholar
25 Cai J , KaramJA, ParviziJ, SmithEB, SharkeyPF. Aquacel surgical dressing reduces the rate of acute PJI following total joint arthroplasty: a case-control study. J Arthroplasty2014;29:1098-1100.CrossrefPubMed Google Scholar
26 Argenta LC , MorykwasMJ. Vacuum-assisted closure: a new method for wound control and treatment: clinical experience. Ann Plast Surg1997;38:563-576.PubMed Google Scholar
27 Fleischmann W , StreckerW, BombelliM, KinzlL. Vacuum sealing as treatment of soft tissue damage in open fractures. Unfallchirurg1993;96:488-492. (In German). Google Scholar
28 Thompson JT , MarksMW. Negative pressure wound therapy. Clin Plast Surg2007;34:673-684.CrossrefPubMed Google Scholar
29 Armstrong DG , LaveryLA, BoultonAJ. Negative pressure wound therapy via vacuum-assisted closure following partial foot amputation: what is the role of wound chronicity?Int Wound J2007;4:79-86.CrossrefPubMed Google Scholar
30 Vig S , DowsettC, BergL, et al.. Evidence-based recommendations for the use of negative pressure wound therapy in chronic wounds: steps towards an international consensus. J Tissue Viability2011;20:S1-S18.CrossrefPubMed Google Scholar
31 Ubbink DT , WesterbosSJ, NelsonEA, VermeulenH. A systematic review of topical negative pressure therapy for acute and chronic wounds. Br J Surg2008;95:685-692.CrossrefPubMed Google Scholar
32 Bovill E , BanwellPE, TeotL, et al.. Topical negative pressure wound therapy: a review of its role and guidelines for its use in the management of acute wounds. Int Wound J2008;5:511-529.CrossrefPubMed Google Scholar
33 Webb LX . New techniques in wound management: vacuum-assisted wound closure. J Am Acad Orthop Surg2002;10:303-311.CrossrefPubMed Google Scholar
34 Karlakki S , BremM, GianniniS, et al.. Negative pressure wound therapy for managementof the surgical incision in orthopaedic surgery: A review of evidence and mechanisms for an emerging indication. Bone Joint Res2013;2:276-284.CrossrefPubMed Google Scholar
35 Morykwas MJ , FalerBJ, PearceDJ, ArgentaLC. Effects of varying levels of subatmospheric pressure on the rate of granulation tissue formation in experimental wounds in swine. Ann Plast Surg2001;47:547-551.CrossrefPubMed Google Scholar
36 Malmsjö M , IngemanssonR, MartinR, HuddlestonE. Negative-pressure wound therapy using gauze or open-cell polyurethane foam: similar early effects on pressure transduction and tissue contraction in an experimental porcine wound model. Wound Repair Regen2009;17:200-205. Google Scholar
37 Borgquist O , IngemanssonR, MalmsjöM. Wound edge microvascular blood flow during negative-pressure wound therapy: examining the effects of pressures from -10 to -175 mmHg. Plast Reconstr Surg2010;125:502-509.CrossrefPubMed Google Scholar
38 Ichioka S , WatanabeH, SekiyaN, ShibataM, NakatsukaT. A technique to visualize wound bed microcirculation and the acute effect of negative pressure. Wound Repair Regen2008;16:460-465.CrossrefPubMed Google Scholar
39 Horch RE , MunchowS, DraguA. Erste Zwischenergebnisse der Perfusions- beeinflussung durch Prevena: gewebsperfusion. DZF2012;16:1-3. (In German). Google Scholar
40 Wilkes RP , KilpadiDV, ZhaoY, KazalaR, McNultyA. Closed incision management with negative pressure wound therapy (CIM): biomechanics. Surg Innov2012;19:67-75.CrossrefPubMed Google Scholar
41 Meeker J , WeinholdP, DahnersL. Negative pressure therapy on primarily closed wounds improves wound healing parameters at 3 days in a porcine model. J Orthop Trauma2011;25:756-761.CrossrefPubMed Google Scholar
42 Glaser DA , FarnsworthCL, VarleyES, et al.. Negative pressure therapy for closed spine incisions: a pilot study. Wounds2012;24:308-316.PubMed Google Scholar
43 Morykwas MJ , ArgentaLC, Shelton-BrownEI, McGuirtW. Vacuum-assisted closure: a new method for wound control and treatment: animal studies and basic foundation. Ann Plast Surg1997;38:553-562.CrossrefPubMed Google Scholar
44 Kamolz LP , AndelH, HaslikW, et al.. Use of subatmospheric pressure therapy to prevent burn wound progression in human: first experiences. Burns2004;30:253-258.CrossrefPubMed Google Scholar
45 Kubiak BD , AlbertSP, GattoLA, et al.. Peritoneal negative pressure therapy prevents multiple organ injury in a chronic porcine sepsis and ischemia/reperfusion model. Shock2010;34:525-534.CrossrefPubMed Google Scholar
46 Young SR , HamptonS, MartinR. Non-invasive assessment of negative pressure wound therapy using high frequency diagnostic ultrasound: oedema reduction and new tissue accumulation. Int Wound J2013;10:383-388.CrossrefPubMed Google Scholar
47 Pachowsky M , GusindeJ, KleinA, et al.. Negative pressure wound therapy to prevent seromas and treat surgical incisions after total hip arthroplasty. Int Orthop2012;36:719-722.CrossrefPubMed Google Scholar
48 Stannard JP , VolgasDA, McGwinGIII, et al.. Incisional negative pressure wound therapy after high-risk lower extremity fractures. J Orthop Trauma2012;26:37-42.CrossrefPubMed Google Scholar
49 Kilpadi DV , CunninghamMR. Evaluation of closed incision management with negative pressure wound therapy (CIM): hematoma/seroma and involvement of the lymphatic system. Wound Repair Regen2011;19:588-596.CrossrefPubMed Google Scholar
50 Matatov T , ReddyKN, DoucetLD, ZhaoCX, ZhangWW. Experience with a new negative pressure incision management system in prevention of groin wound infection in vascular surgery patients. J Vasc Surg2013;57:791-795.CrossrefPubMed Google Scholar
51 Timmons J , RussellF. Introducing a new portable negative pressure wound therapy (NPWT) system. Wounds UK2012;8:47-54. Google Scholar
52 Hudson DA , AdamsKG, HuyssteenAV, MartinR, HuddlestonEM. Simplified negative pressure wound therapy: clinical evaluation of an ultraportable, no-canister system. Int Wound J2015;12:195-201.CrossrefPubMed Google Scholar
53 Schulz KF , AltmanDG, MoherD; CONSORT Group. CONSORT 2010 statement: updated guidelines for reporting parallel group randomised trials. Int J Surg2011;9:672-677.CrossrefPubMed Google Scholar
54 Zhou XH , DinhP. Nonparametric confidence intervals for the one-and two-sample problems. Biostatistics2005;6:187-200. Google Scholar
55 Cheung G , CarmontMR, BingAJ, et al.. No drain, autologous transfusion drain or suction drain? A randomised prospective study in total hip replacement surgery of 168 patients. Acta Orthop Belg2010;76:619-627.PubMed Google Scholar
56 No authors listed. Department of Health Reference Costs 2011-2012. https://www.gov.uk/government/publications/nhs-reference-costs-financial-year-2011-to-2012 (date last accessed 24 May 2016). Google Scholar
57 No authors listed. National Joint Registry 11th Annual Report2014. http://www.njrcentre.org.uk/njrcentre/Portals/0/Documents/England/Reports/11th_annual_report/NJR%2011th%20Annual%20Report%202014.pdf (date last accessed 24 May 2016). Google Scholar
58 Shantz JA , VernonJ, LeiterJ, MorshedS, StrangesG. Sutures versus staples for wound closure in orthopaedic surgery: a randomized controlled trial. BMC Musculoskelet Disord2012;13:89.CrossrefPubMed Google Scholar
59 Smith TO , SextonD, MannC, DonellS. Sutures versus staples for skin closure in orthopaedic surgery: meta-analysis. BMJ2010;340:c1199.CrossrefPubMed Google Scholar
60 Khan RJ , FickD, YaoF, et al.. A comparison of three methods of wound closure following arthroplasty: a prospective, randomised, controlled trial. J Bone Joint Surg [Br]2006;88-B:238-242.CrossrefPubMed Google Scholar
61 Howell RD , HadleyS, StraussE, PelhamFR. Blister formation with negative pressure dressings after total knee arthroplasty. Curr Orthop Pract2011;22:176-179. Google Scholar
