




Abstract
Objective
Hip arthroscopy in the setting of hip dysplasia is controversial in the orthopaedic community, as the outcome literature has been variable and inconclusive. We hypothesise that outcomes of hip arthroscopy may be diminished in the setting of hip dysplasia, but outcomes may be acceptable in milder or borderline cases of hip dysplasia.
Methods
A systematic search was performed in duplicate for studies investigating the outcome of hip arthroscopy in the setting of hip dysplasia up to July 2015. Study parameters including sample size, definition of dysplasia, outcomes measures, and re-operation rates were obtained. Furthermore, the levels of evidence of studies were collected and quality assessment was performed.
Results
The systematic review identified 18 studies investigating hip arthroscopy in the setting of hip dysplasia, with 889 included patients. Criteria used by the studies to diagnose hip dysplasia and borderline hip dysplasia included centre edge angle in 72% of studies but the range of angles were quite variable. Although 89% of studies reported improved post-operative outcome scores in the setting of hip dysplasia, revision rates were considerable (14.1%), with 9.6% requiring conversion to total hip arthroplasty.
Conclusion
The available orthopaedic literature suggests that although improved outcomes are seen in hip arthroscopy in the setting of hip dysplasia, there is a high rate of re-operation and conversion to total hip arthroplasty. Furthermore, the criteria used to define hip dysplasia vary considerably among published studies.
Cite this article: M. Yeung, M. Kowalczuk, N. Simunovic, O. R. Ayeni. Hip arthroscopy in the setting of hip dysplasia: A systematic review. Bone Joint Res 2016;5:225–231. DOI: 10.1302/2046-3758.56.2000533.
Article focus
-
The surgical outcomes of hip arthroscopy in the setting of hip dysplasia.
-
Outcomes of hip arthroscopy are inferior in dysplastic compared with non-dysplastic patients, although outcomes may be better in borderline dysplastic patients compared with dysplastic patients.
Key messages
-
Definitions of dysplasia and borderline dysplasia are inconsistent and variable.
-
Higher rates of re-operation and conversion to total hip arthroplasty in patients with hip dysplasia.
-
Further high-quality studies are needed to determine hip arthroscopy outcomes at differing severities of hip dysplasia.
Strengths and limitations
-
Broad and comprehensive systematic review of databases performed in duplicate.
-
Inconsistency of dysplasia definitions in literature preclude formal analysis.
Introduction
Over the past decade, hip arthroscopy has become an increasingly common orthopaedic procedure, indicated to treat pathologies such as femoroacetabular impingement (FAI) and symptomatic labral tears.1,2 Satisfactory surgical outcomes have been achieved for these indications.3 However, the indications and outcomes of hip arthroscopy in the setting of hip dysplasia or borderline hip dysplasia have been inconclusive and controversial.4,5
Similar to femoroacetabular impingement, hip dysplasia has been implicated as a factor for the development of osteoarthritis in the hip.6 It is postulated that the decreased bony coverage from hip dysplasia results in higher contact stresses in the hip joint, leading to cartilage and labral degeneration, and ultimately osteoarthritis.7 Historically, hip preservation surgery for hip dysplasia has been limited to open procedures such as periacetabular osteotomies (PAO). Orthopaedic literature has shown that PAOs are an effective technique in the treatment of symptomatic hip dysplasia, with excellent results even in long-term follow-up.8 Hip arthroscopy has been used as an adjunctive procedure, undertaken concomitantly with a PAO to treat intra-articular hip pathology, with positive outcomes.9 However, isolated hip arthroscopy in the setting of hip dysplasia has shown variable outcomes in the literature. Some studies have demonstrated good outcomes, emphasising that outcomes were more correlated with the type of intra-articular pathology, independent of the presence of dysplasia.4 Other studies presented poor outcomes, suggesting that hip arthroscopy is not beneficial in dysplastic patients and that the surgery may even accelerate the arthritic process.5
The goal of this systematic review was to assess the indications and outcomes of isolated hip arthroscopy in the setting of hip dysplasia. We hypothesised that the definitions of hip dysplasia used as indications for hip arthroscopy are variable, and that the outcomes of hip arthroscopy are less predictable in the setting of hip dysplasia, although outcomes may be improved in the setting of mild or borderline dysplasia.
Materials and Methods
Search Strategy
Electronic databases (MEDLINE, EMBASE, PUBMED and Cochrane Library) were searched for surgical hip arthroscopy studies in their entirety up to July 2015, when the search was performed. The search strategy used the following search terms: “hip dysplasia” or “developmental dysplasia of the hip”, “congenital hip dysplasia”, “acetabular dysplasia”, “hip instability”, AND “hip arthroscopy”, “arthroscopy”, or “hip” AND “arthroscopy”. The ‘congenital hip dislocation’, ‘hip dislocation’, ‘hip dysplasia’, ‘hip arthroscopy’, ‘arthroscopic surgery’ and ‘Hip [Surgery]’ subheadings in EMBASE and the ‘Hip Dislocation, Congenital’ and ‘Arthroscopy’ subheadings in MEDLINE were also included in the search (see Table i, supplementary material). Relevant conference proceedings, abstracts, and reference lists of the resulting full-text articles were hand-searched for pertinent articles. The results were uploaded to a bibliographical management database (RefWorks, Version 2.0, 2009, Proquest, Ann Arbour, Michigan).
Inclusion and exclusion criteria
The search results were screening in duplicate using pre-specified eligibility criteria. The inclusion criteria for this systematic review were:
-
studies of human patients of all ages and gender;
-
studies reporting surgical outcomes of isolated hip arthroscopy in the setting of hip dysplasia;
-
studies with all included patients having the diagnosis of hip dysplasia or borderline hip dysplasia, excluding a designated control group, and;
-
studies of all languages.
Exclusion criteria were: review articles, diagnostic studies, case reports and studies with fewer than five patients, studies that only reported intra-operative findings with no post-operative outcomes, studies investigating hip arthroscopy in conjunction with open procedures such as osteotomies, paediatric studies investigating arthroscopically assisted reduction of developmental hip dysplasia and studies reporting selected hip arthroscopy cases with inclusion criteria based on poor outcome or complications that would bias this study (e.g. study strictly reporting failed hip arthroscopy cases that required further osteotomy, but does not include ‘successful’ cases not requiring revision from the same cohort). Any discrepancies in terms of inclusion were resolved through discussion and consensus between reviewers.
Data collection
Data were collected from the included articles by two reviewers. Abstracted data included the following information: title, author, year of publication, location, sample size, number of male and female patients, mean age, length of follow-up, levels of evidence, type of surgical procedure, study definition of hip dysplasia, surgical outcomes, complications, and revisions. Studies were rated according to the levels of evidence: randomised controlled trials were considered Level I, non-randomised prospective comparative studies were considered level II studies, retrospective comparative studies or case control studies were considered level III evidence, and case series were considered Level IV evidence.
Study quality was assessed in duplicate by two co-authors (MY and MK). The quality assessment scoring for non-randomised studies was performed using the Methodological Index for Non-Randomized Studies (MINORS) instrument.10 Items were scored 0 (not reported), 1 (reported but inadequate) and 2 (reported and adequate). The following items were scored for all non-randomised studies: a clearly stated aim, inclusion of consecutive patients, prospective collection of data, endpoints appropriate to the aim of the study, unbiased assessment of the study endpoint, follow-up period appropriate to the aim of the study, loss to follow-up less than 5%, and prospective calculation of sample size. The following additional categories were scored for comparative studies: adequate control group, contemporary groups, baseline equivalence of groups, adequate statistical analyses. As adapted from Braga et al,11 the methodological quality of the studies was rated based on the MINORS criteria: studies that met < 25% of the score criteria were considered very low methodological quality; between 25% and 49% of the criteria were considered low methodological quality; between 50% and 74% of the criteria considered moderate methodological quality; and > 75% of the criteria considered high methodological quality.
Statistical analysis
The κ (kappa) statistic was used to examine inter-observer agreement for study eligibility. On the basis of the guidelines of Landis and Koch,12 a kappa of 0 to 0.2 represents slight agreement; 0.21 to 0.40, fair agreement; 0.41 to 0.60, moderate agreement; and 0.61 to 0.80, substantial agreement. A value above 0.80 is considered almost perfect agreement.
Results
Study identification
The electronic searches yielded 1227 studies, with 839 studies remaining following removal of duplicates. Following title, abstract and full-text reviews, 18 studies were found to meet the inclusion criteria and were included in the analysis (Fig. 1). Statistical agreement analysis showed a kappa value of 0.956 (95% confidence interval (CI) 0.949 to 0.961) for the title and abstract screen, and a kappa value of 0.967 (95% CI 0.932 to 0.983) for the full-text review, which indicated almost perfect agreement between reviewers. Included in the study were 12 case series, five retrospective comparative studies, one prospective cohort study. There were no randomised controlled trials.
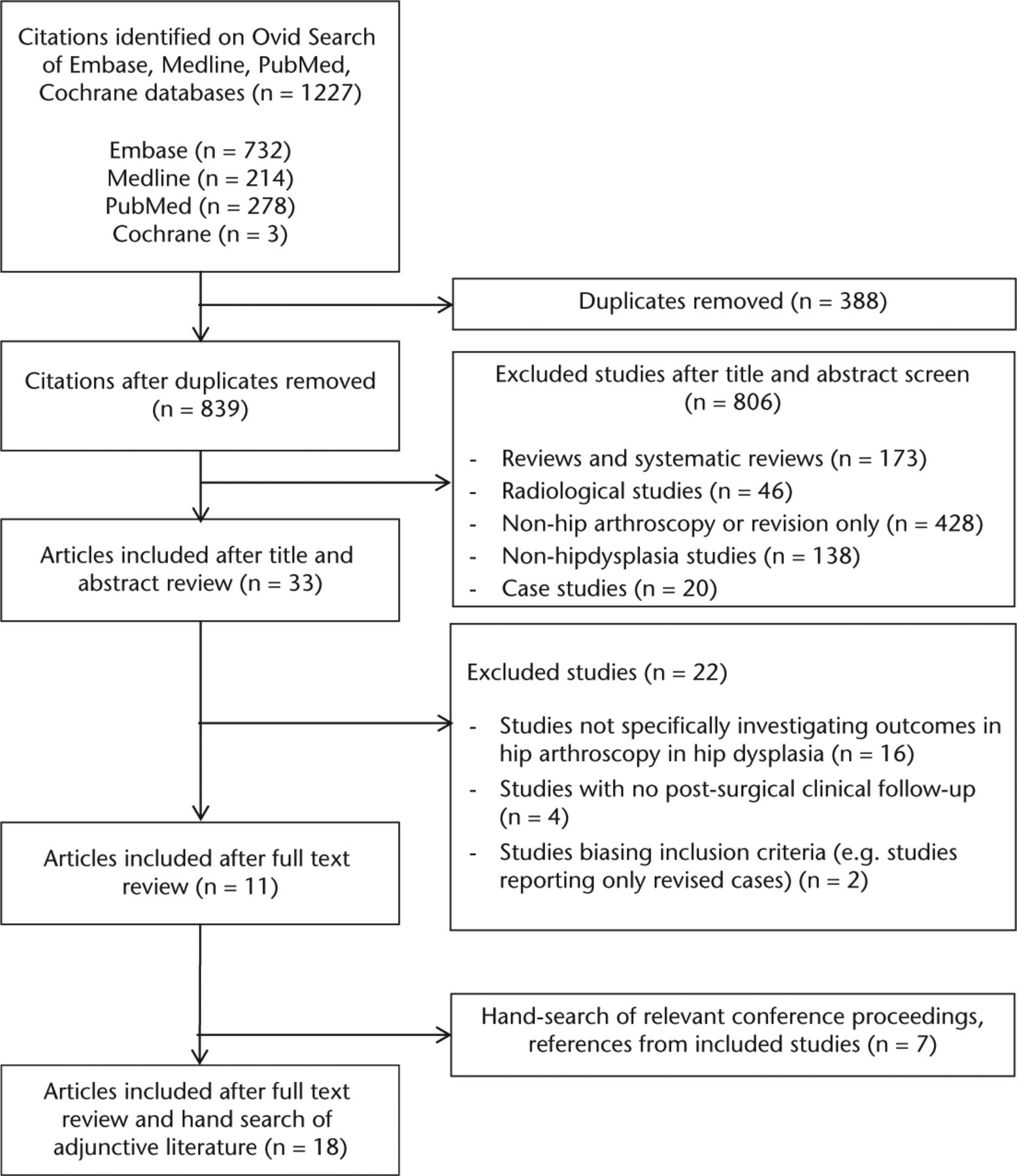
Fig. 1
Summary of the literature search and inclusion/exclusion process.
Study characteristics
All of the included studies were published between 1998 and 2015. A total sample size of 889 patients with 949 hips from the included studies underwent hip arthroscopy in the setting of hip dysplasia. Across the 18 included studies, the mean patient age after adjustment for the sample size of each study was 35.4 years. Follow-up periods of the included studies ranged from six months to 14 years. Mean follow-up (of studies that provided a mean follow-up length) was 32.2 months after adjustment for sample size of each study. The most common procedures performed were labral repair (number of patients = 258, 27.2%), femoral osteochondroplasty (n = 240, 25.3%), capsular plication (n = 150, 15.8%), labral debridement (n = 149, 15.7%), capsular closure (n = 142, 15.05%), and ligamentum teres debridement (n = 121, 12.8%). Common outcome measurement tools used included the Modified Harris hip score (mHHS) (n = 12, 66.7%), patient satisfaction (n = 5, 27.8%), the Non-Arthritis Hip Score (NAHS) (n = 3 16.7%) and the Hip Outcome Score (HOS) (n = 3, 16.7%). Study characteristics are described in Table I.
Table I.
Characteristics of included studies
| Characteristics of included studies | |
|---|---|
| Number of studies | 18 |
| Number of included patients | 889 (949 hips) |
| Mean age of patients | 35.4 yrs |
| Duration of follow-up | 32.2 mths (6 mths to 14 yrs) |
| Type of studies (number of studies) | |
| Randomised controlled trial | 0 (0.0) |
| Prospective comparative study | 1 (5.6) |
| Retrospective comparative study | 5 (27.8) |
| Case series | 12 (66.7) |
| Country of publication (number of studies) | |
| United States | 12 (66.7) |
| Japan | 4 (22.2) |
| United Kingdom | 2 (11.1) |
| Procedures performed during hip arthroscopy* (number of patients) | |
| Labral repair | 258 (27.2) |
| Femoral osteochondroplasty | 240 (25.3) |
| Capsular plication | 150 (15.8) |
| Labral debridement | 149 (15.7) |
| Capsular closure | 142 (15.0) |
| Ligamentum teres debridement | 121 (12.8) |
| Subspine resection | 104 (11.0) |
| Microfracture | 44 (4.6) |
| Chondroplasty | 34 (3.6) |
| Acetabular rim trimming | 22 (2.3) |
| Endoscopic shelf acetabuloplasty | 17 (1.8) |
| Iliopsoas tendon debridement | 15 (1.5) |
| Loose body removal | 8 (0.8) |
| Labral reconstruction | 4 (0.4) |
| Pulvinar debridement | 3 (0.3) |
| Trochanteric bursectomy | 1 (0.1) |
| Thermal capsulorrhaphy | 1 (0.1) |
| Data for other procedures performed not provided | 383 (40.36) |
| Outcome measure tools used (number of studies) | |
| Modified Harris hip score (mHHS) | 12 (66.7) |
| Patient satisfaction | 5 (27.8) |
| Non-Arthritic Hip Score (NAHS) | 3 (16.7) |
| Hip Outcome Score (HOS) (Activity of daily living and sports specific) | 3 (16.7) |
| Harris hip score (HHS) | 1 (5.6) |
| Hip disability and Osteoarthritis Outcome Score (HOOS) | 1 (5.6) |
| Super Simple Hip Score (SUSHI) | 1 (5.6) |
| Western Ontario/McMaster Osteoarthritis Index (WOMAC) | 1 (5.6) |
| Short Form (SF) 36 | 1 (5.6) |
| Pain visual analogue score | 1 (5.6) |
| International Hip Outcome Tool (iHOT) | 1 (5.6) |
-
*
Percentages do not add up to 100% as some cases have multiple procedures done
Criteria for hip dysplasia
The criteria of hip dysplasia or borderline hip dysplasia used in the included studies are described in Table II. A total of 13 (72%) of the studies used the centre edge angle (CEA) (of Wiberg)13 as their criterion for hip dyplasia or borderline dysplasia. Nine studies included the criteria for borderline or mild hip dysplasia in their methodology and inclusions: four studies used a CEA of 20° to 25° as a criterion for borderline hip dysplasia; two studies used a CEA of 18° to 25°; two studies used a CEA of 22° to 28°; while one study used a CEA of < 25° in conjunction with an anterior CEA of < 25° or Sharp angle < 40° as their criteria. Of the nine studies that included a criterion for hip dysplasia or moderate hip dysplasia, three studies used a CEA of < 20°, two studies used a CEA of 16° to 22°, one study used a CEA of < 25°, one study used a CEA of 16° to 24°, one study used a CEA of 19° to 27°, and one study used an acetabular index of < 20° or anterior or posterior undercoverage of the femoral head of < 10%. Of the 18 studies, four studies did not provide specific radiographic criteria for the diagnosis of hip dysplasia or borderline dysplasia.
Table II.
Radiographic definitions of hip dysplasia and borderline dysplasia in included studies
| Radiographic criteria for hip dysplasia | Studies used (%) |
|---|---|
| Borderline or mild dysplasia | 9 (50) |
| - Centre edge angle of 20° to 25° | 4 (22.2) |
| - Centre edge angle of 18° to 25° | 2 (11.1) |
| - Centre edge angle of 22° to 28° | 2 (11.1) |
| - Centre edge angle of 25° or anterior CEA of 25° or Sharp angle less than 40° | 1 (5.6) |
| General or moderate hip dysplasia | 9 (50) |
| - Centre edge angle < 20° | 3 (16.7) |
| - Centre edge angle of 16° to 22° | 2 (11.1) |
| - Centre edge angle of < 25° | 1 (5.6) |
| - Centre edge angle of 16° to 24° | 1 (5.6) |
| - Centre edge angle of 19° to 27° | 1 (5.6) |
| - acetabular index of < 20° or anterior or posterior undercoverage of the femoral head of < 10% | 1 (5.6) |
| No radiographic criteria provided | 4 (22.2) |
Surgical outcomes in dysplastic versus non-dysplastic patients
Six studies compared the outcomes of hip arthroscopy in dysplastic patients compared with a non-dysplastic cohort.14-19 All six studies found improvement in post-operative mHHS,14-17,19 NAHS,18 International Hip Outcome Tool (iHOT)16 and HOS16 measures in the dysplastic cohort. The studies by Jayasekera, Aprato and Villar,14 Kalore and Jiranek15 and Nawabi et al16 did not find any significant difference in improvement of outcome scores between the dysplastic and non-dysplastic cohorts. In contrast, the studies by Larson et al,17 Matsuda,18 and Shimizu19 found significantly worse outcomes in their dysplastic cohort compared with the non-dysplastic cohort. Both the studies from Kalore and Jiranek15 and Matsuda18 noted a higher re-operation rate and THA conversion rate in the dysplastic group. Similarly, Larson et al17 found that the dysplastic cohort had an increased rate of failure compared with the non-dysplastic group (see Table ii, in supplementary material).
Surgical outcomes in borderline dysplasia versus moderate dysplasia
Four studies classified patients into borderline dysplasia and moderate dysplasia categories. Briggs20 concluded that there was no association between mean improvement in mHHS and CEA, nor between borderline dysplastic (CEA 20° to 25°) and dysplastic (CEA < 20°) categories. Similarly, in the study by Byrd and Jones,4 no statistical difference was found in the improvement of mHHS scores between borderline dysplastic (CEA 20° to 25°) and dysplastic patients (CEA < 20°). However, the study by McCarthy and Lee21 found that the total hip arthroscopy (THA) conversion rate of 54% in dysplastic patients (CEA 16° to 22°) was considerably higher than the 3% rate in borderline dysplastic patients (CEA 22° to 28°). The study by Dwyer, Lee and McCarthy22 did classify their patients into groups of dysplasia (CEA 16° to 22°) and borderline dysplasia (CEA 22° to 28°) and but did not make any comparisons between the two. Given the different CEA ranges used by the studies to classify the severity of dysplasia, a formal compilation of the data was not performed.
Failures, re-operations and complications in hip arthroscopy in the setting of hip dysplasia
Within the cumulative sample size of 949 dysplastic or borderline dysplastic hips included in this systematic review, 134 cases (14.1%) required a revision procedure due to persistence of symptoms or clinical worsening. A total of 90 cases (9.5%) required conversion to total hip arthroplasty, although this number is likely underestimated as some studies provided a re-operation rate but did not specify the procedure. Of the five studies that provided a time from initial hip arthroscopy to hip arthroplasty, the mean time to conversion to total hip arthroplasty was 29.4 months when adjusted for study sample size. Furthermore, 18 hips (1.9%) required further revision arthroscopy, seven patients (0.7%) required subsequent periacetabular osteotomy, and seven patients (0.7%) underwent subsequent revision with open femoral osteochondroplasty. Other complications were not commonly reported in the studies included in this systematic review; one study reported a case of lateral femoral cutaneous nerve palsy.23
Quality assessment
Quality assessment scoring of the non-randomised studies in this systematic review was performed using the MINORS criteria. Of the nine studies that were suitable for quality assessment, there were seven non-comparative studies and two comparative studies. Of the seven non-comparative studies, the mean consensus scoring was calculated to be 9.1/16; one study was considered of high methodological quality, five studies were of moderate quality, and one study was considered very low quality. Of the two comparative studies, the mean consensus scoring was calculated to be 17/24; both studies were of moderate methodological quality. Given that the full-text results of the other nine included studies (from abstracts and conference proceedings) were not available, it was not feasible to perform quality assessment scoring using the MINORS criteria as intended or with the use of another quality assessment tool.
With regard to level of evidence, of the 18 included studies, one study was of level II evidence (e.g. prospective comparative study), five studies were of level III evidence (retrospective comparative study) and 12 studies were of level IV evidence (case series). There were no studies of level I evidence (e.g. randomised controlled trials).
Discussion
Key findings
One of the purposes of this study was to investigate the hip arthroscopy outcomes of patients with dysplastic hips. The majority of the studies in this systematic review showed improvement in outcome measures post-operatively. One study showed some short-term improvement followed by worsening of outcome measures.5 However, in this study labral repairs were not performed on any of the patients, and only debridement was performed.5 Although in this study the pathology may not have indicated a repair, the studies of both Larson et al17 and Domb et al24 suggest that labral repair and capsular plication were predictive of improved outcomes in the dysplastic hip patient population. This systematic review was not conclusive with regard to whether outcomes in dysplastic patients are comparable with, or worse than, those of non-dysplastic patients, as three comparative studies found no difference between groups while three other studies found that outcomes were worse in dysplastic patients.
However, in spite of the optimistic findings of improved post-operative outcome measures, this systematic review also found that re-operation rates were considerable, suggesting that although dysplastic patients improved with hip arthroscopy, many of them required revision procedures and/or conversion to total hip arthroplasty. In this systematic review of dysplastic patients, the re-operation rate increased more than twofold and the THA conversion rate increased over threefold when compared with a previous systematic review which showed a re-operation rate of 6.3% and THA conversion rate of 2.9% in the general hip arthroscopy population.25
This systematic review sought to determine whether outcomes were comparable between dysplastic and borderline dysplastic patients. It was hypothesised that better outcomes would be seen in borderline dysplastic patients. The evidence appears to be inconclusive, as two studies suggest outcomes were comparable between borderline and dysplastic groups, whereas another study found a significantly higher rate of failure and re-operation in the dysplastic group. One possible reason for this discrepancy in findings may be related to the variability of criteria used in defining dysplasia and borderline dysplasia. As hypothesised, this systematic review found that although the majority of studies used a common measure (CEA) to define dysplasia, the specific range of angles used between studies was quite variable. In fact, there was considerable overlap and inconsistency between what the studies considered borderline versus moderate hip dysplasia. Consequently, there was difficulty in compiling and interpreting what severity of dysplasia is indicated or contraindicated for hip arthroscopy, given these discrepancies. These results suggest that there is a need for more consistent criteria in defining borderline versus moderate versus severe hip dysplasia.
This systematic review had several strengths. Firstly, a broad inclusive search strategy of multiple databases was used, followed by a hand-search of referenced articles, recent conference proceedings and abstracts. Furthermore, study screening, data abstraction and quality assessment scoring were performed by multiple reviewers in order to reduce sources of bias.
However, there were limitations to our study. The variability of the criteria of borderline and moderate hip dysplasia precluded any formal analysis or comparison of the outcomes of hip arthroscopy in the setting of differing severity of hip dysplasia. Likewise, given that some of our included studies were preliminary data from abstracts and conference proceedings, the complete methodology was not available to perform quality assessment scoring on those studies.
Future directions
Although most studies agree that patients with hip dysplasia do benefit from some arthroscopic procedures, the evidence varies on whether these outcomes are worse compared than for non-dysplastic patients. This study does show that re-operation and THA conversion rates are higher in dysplastic patients. Some recent studies, however, have suggested that positive outcomes are associated with arthroscopic labral repair and capsular plication.15,24 Further high-quality studies are required to determine whether newer arthroscopic techniques such as capsular plication and repair are responsible for improved outcomes in dysplastic hips.
Furthermore, the evidence is still controversial with regard to whether hip arthroscopy leads to better outcomes in borderline dysplasia than in moderately dysplastic hips. There is evidence to suggest that there is a certain level of borderline dysplasia (as determine by CEA), where good outcomes can be obtained, and more severe levels of dysplasia where arthroscopic outcomes may be poor.21 More high-quality trials are needed to further investigate the outcomes of hip arthroscopy in various levels of dysplasia. These studies should compare results based on severity of dysplasia in order to better determine its influence on outcomes. Additionally, further studies and discussions to delineate consensus definitions of dysplasia and borderline dysplasia may facilitate future relevant research studies. These areas of further exploration will provide clinicians with improved guidelines regarding the indications for hip arthroscopy in patients with dysplastic hips, and the appropriate arthroscopic techniques that will lead to improved outcomes in these patients.
In conclusion, the results of this systematic review indicate that although improvement of post-operative outcomes is seen in hip arthroscopy in the setting of hip dysplasia, there is a higher rate of re-operation and conversion to total hip arthroplasty compared with non-dysplastic hips. It was also found that the criteria for hip dysplasia used in the hip arthroscopy literature are quite variable, and it remains to be determined whether improved outcomes are achieved in patients with borderline dysplasia compared with moderate dysplasia.
Supplementary material
Tables showing database search strategies and the characteristics, criteria of dysplasia, results and re-operations in included studies, are available alongside the online version of this article at www.bjr.boneandjoint.org.uk
Funding Statement
None declared.
ICMJE conflict of interest
O. R. Ayeni is an Editorial board member for Knee Surgery, Sports Traumatology, Arthroscopy and the American Journal of Sports Medicine, and also reports speakers bureau membership for Conmed and Smith & Nephew (no payment).
References
1 Colvin AC , HarrastJ, HarnerC. Trends in hip arthroscopy. J Bone Joint Surg [Am]2012;94-A:e23.CrossrefPubMed Google Scholar
2 Bozic KJ , ChanV, ValoneFHIII, FeeleyBT, VailTP. Trends in hip arthroscopy utilization in the United States. J Arthroplasty2013;28(Suppl):140-143.CrossrefPubMed Google Scholar
3 Philippon MJ , BriggsKK, YenYM, KuppersmithDA. Outcomes following hip arthroscopy for femoroacetabular impingement with associated chondrolabral dysfunction: minimum two-year follow-up. J Bone Joint Surg [Br]2009;91-B:16-23.CrossrefPubMed Google Scholar
4 Byrd JW , JonesKS. Hip arthroscopy in the presence of dysplasia. Arthroscopy2003;19:1055-1060.CrossrefPubMed Google Scholar
5 Parvizi J , BicanO, BenderB, et al.. Arthroscopy for labral tears in patients with developmental dysplasia of the hip: a cautionary note. J Arthroplasty2009;24(Suppl):110-113.CrossrefPubMed Google Scholar
6 Jacobsen S , Sonne-HolmS, SøballeK, GebuhrP, LundB. Hip dysplasia and osteoarthrosis: a survey of 4151 subjects from the Osteoarthrosis Substudy of the Copenhagen City Heart Study. Acta Orthop2005;76:149-158.CrossrefPubMed Google Scholar
7 Mavcic B , IglicA, Kralj-IglicV, BrandRA, VengustR. Cumulative hip contact stress predicts osteoarthritis in DDH. Clin Orthop Relat Res2008;466:884-891.CrossrefPubMed Google Scholar
8 Steppacher SD , TannastM, GanzR, SiebenrockKA. Mean 20-year followup of Bernese periacetabular osteotomy. Clin Orthop Relat Res2008;466:1633-1644.CrossrefPubMed Google Scholar
9 Kim KI , ChoYJ, RamtekeAA, YooMC. Peri-acetabular rotational osteotomy with concomitant hip arthroscopy for treatment of hip dysplasia. J Bone Joint Surg [Br]2011;93-B:732-737.CrossrefPubMed Google Scholar
10 Slim K , NiniE, ForestierD, et al.. Methodological index for non-randomized studies (minors): development and validation of a new instrument. ANZ J Surg2003;73:712-716.CrossrefPubMed Google Scholar
11 Braga LH , MijovicH, FarrokhyarF, et al.. Antibiotic Prophylaxis for Urinary Tract Infections in Antenatal Hydronephrosis. Pediatrics2013;131:e251.CrossrefPubMed Google Scholar
12 Landis JR , KochGG. The measurement of observer agreement for categorical data. Biometrics1977;33:159-174.PubMed Google Scholar
13 Wiberg G . Shelf operation in congenital dysplasia of the acetabulum and in subluxation and dislocation of the hip. J Bone Joint Surg [Am]1953;35-A:65–80.PubMed Google Scholar
14 Jayasekera N , ApratoA, VillarRN. Hip arthroscopy in the presence of acetabular dysplasia. Open Orthop J2015;9:185-187.CrossrefPubMed Google Scholar
15 Kalore NV , JiranekWA. Save the torn labrum in hips with borderline acetabular coverage. Clin Orthop Relat Res2012;470:3406-3413.CrossrefPubMed Google Scholar
16 Nawabi DH , BediA, RanawatAS, KellyBT. Outcomes of hip arthroscopy for patients with symptomatic borderline dysplasia: a comparison to a matched cohort of patients with symptomatic FAI. Orthop J Sports Med2015;3(suppl). Google Scholar
17 Larson C , RossJ, StoneR, et al.. Arthroscopic management of dysplastic hip morphologies: predictors of success and failures and comparison to an arthroscopic FAI cohort. Arthroscopy2015;31(Suppl):14. Google Scholar
18 Matsuda DK . Arthroscopic surgical outcomes of mild dysplasia versus focal pincer femoroacetabular impingement: a multicenter case control study [abstract]ISHA, 2014. Google Scholar
19 Shimizu J . Arthroscopic hip surgery for borderline dysplasia-surgical outcomes compared with cohort after arthroscopic FAI correction [abstract]. ISAKOS, 2015. Google Scholar
20 Briggs KK . Hip arthroscopy in the adult dysplastic hip [abstract]. Annual Scientific Meeting of the International Society for Hip Arthroscopy, 2011. Google Scholar
21 McCarthy JC , LeeJA. Acetabular dysplasia: a paradigm of arthroscopic examination of chondral injuries. Clin Orthop Relat Res2002;405:122-128.CrossrefPubMed Google Scholar
22 Dwyer MK , LeeJA, McCarthyJC. Cartilage status at time of arthroscopy predicts failure in patients with hip dysplasia. J Arthroplasty2015;30(Suppl):121-124.CrossrefPubMed Google Scholar
23 Uchida S . New surgical technique of arthroscopic shelf acetabuloplasty combined with labral repair and cam osteochondroplasty for the patients with dysplasia of the hip [abstract]. ISHA, 2012. Google Scholar
24 Domb BG , StakeCE, LindnerD, El-BitarY, JacksonTJ. Arthroscopic capsular plication and labral preservation in borderline hip dysplasia: two-year clinical outcomes of a surgical approach to a challenging problem. Am J Sports Med2013;41:2591-2598.CrossrefPubMed Google Scholar
25 Harris JD , McCormickFM, AbramsGD, et al.. Complications and reoperations during and after hip arthroscopy: a systematic review of 92 studies and more than 6,000 patients. Arthroscopy2013;29:589-595.CrossrefPubMed Google Scholar
