





Abstract
Total hip replacement causes a short-term increase in the risk of mortality. It is important to quantify this and to identify modifiable risk factors so that the risk of post-operative mortality can be minimised. We performed a systematic review and critical evaluation of the current literature on the topic. We identified 32 studies published over the last 10 years which provide either 30-day or 90-day mortality data. We estimate the pooled incidence of mortality during the first 30 and 90 days following hip replacement to be 0.30% (95% CI 0.22 to 0.38) and 0.65% (95% CI 0.50 to 0.81), respectively. We found strong evidence of a temporal trend towards reducing mortality rates despite increasingly co-morbid patients. The risk factors for early mortality most commonly identified are increasing age, male gender and co-morbid conditions, particularly cardiovascular disease. Cardiovascular complications appear to have overtaken fatal pulmonary emboli as the leading cause of death after hip replacement.
Cite this article: Bone Joint Res 2014;3:175–82
Introduction
The capacity for total hip replacement (THR) to improve pain, quality of life and functional outcomes, is widely recognised.1 All surgery carries risk of some kind, including death. In THR performed to treat osteoarthritis in England and Wales, the risk of death in the 90 days following surgery is less than 1%.2 Despite the clarity of mortality as an endpoint, its rarity in the immediate post-operative period makes it difficult to investigate, particularly within medium and small cohort studies. However, risk of death is of paramount importance to patients, their significant others and to healthcare providers. The risk of post-operative death needs to be accurately quantified and conveyed to patients in order to aid decision-making prior to surgery. In addition, modifiable patient and surgical risk factors should be identified, so that measures can be taken to address these factors. We aim to provide an overview of the current knowledge on mortality after THR by means of a systematic review of the literature.
Materials and Methods
Our review team used a rigorous systematic approach, following Meta-analysis Of Observational Studies in Epidemiology (MOOSE) guidelines,3 for the critical evaluation of studies relating to mortality following THR. The primary outcome measures of this review are 30- and 90-day mortality rates, as these are commonly reported mortality indicators.
We included studies published in the English language quoting 30- or 90-day mortality following THR. Studies of mortality that only examined specific subgroups of patients undergoing joint replacement (such as THR for hip fracture, metastatic disease, revision joint replacement, mortality among patients with diabetes or rheumatoid arthritis, or extremes of age) were excluded. Studies quoting ‘in-hospital’ mortality or other data without specific 30- or 90-day mortality rates, were also excluded. In addition, we did not include comparative studies quoting only subgroup mortality data, as part of an investigation into the impact of a novel intervention on mortality, for example a thromboprophylaxis regime or rehabilitation programme. We did include studies reporting mortality following THR for osteoarthritis only, as > 95% of all THRs are performed for osteoarthritis.4 Given the known temporal change in mortality rates, we limited our searches to publications within the last 10 years, since January 2003. The largest study of mortality after THR is, to our knowledge, an 18-year longitudinal study from the USA published in 2011. It contained data from 1 453 493 patients following THR between 1991 and 2008. We only included the most recent cohort of 209 945 patients because of the volume of historical data presented.5
Search strategy
We searched MEDLINE (1 January 2003 to 4 October 2013), and EMBASE (2003 to 2013 Week 39), CAB Abstracts 2003 to 2013 Week 39, and AMED (Allied and Complementary Medicine) 2003 to September 2013. Using controlled vocabulary, we searched the terms, “mortality”, “hip”, and “replacement or arthroplasty”. Further details of the search strategy are shown in Table I. We also searched the reference lists of articles identified by this search strategy and included additional studies deemed relevant. We selected publications from the past 10 years, but also considered commonly referenced and highly regarded older publications.
Table I
Literature search* strategy
| Search Term† | No. of records | ||
|---|---|---|---|
| 1 | hip.tw | 214 308 | |
| 2 | mortality.tw | 1 201 544 | |
| 3 | fracture.mp. [mp=ab, hw, ti, ot, bt, sh, tn, dm, mf, dv, kw, nm, kf, ps, rs, an, ui]† | 396 656 | |
| 4 | arthroplasty.tw | 74 247 | |
| 5 | replacement.tw | 422 949 | |
| 6 | 2 and 1 | 8 662 | |
| 7 | 4 or 5 | 483 770 | |
| 8 | 6 and 7 | 1 981 | |
| 9 | 8 not 3 | 1 206 | |
| 10 | limit 9 to yr=”2003 – Current” | 890 | |
| 11 | limit 10 to English language | 842 | |
| 12 | Removal of duplicates | 484 | |
-
*Search performed on 4th October 2013: We searched MEDLINE (2003 to present), and EMBASE (2003 to 2013 Week 39), CAB Abstracts 2003 to 2013 Week 39, and AMED (Allied and Complementary Medicine) 2003 to September 2013. † Medline search vocabulary: tw, text word; mp, multi-purpose; ab, abstract; hw, heading word; ti, title; ot, original title; bt, broad terms; sh, MeSH subject heading; tn, drug trade name; dm, device manufacturer; mf, drug manufacturer; dv, device trade name; kw, keyword heading; nm, name of substance word; kf, keyword heading word; ps, protocol supplementary concept; rs, rare disease supplementary concept; an, accession number; ui, unique identifier; yr, year of publication
Screening
A total of 484 records were identified from searching the literature; two reviewers independently screened the titles and abstracts of these records to identify potentially useful articles for inclusion in this systematic review. After screening, 32 studies were included and contributed data towards our aggregate estimate of mortality. A flow diagram of the progression of studies through this systematic review is provided in Figure 1.
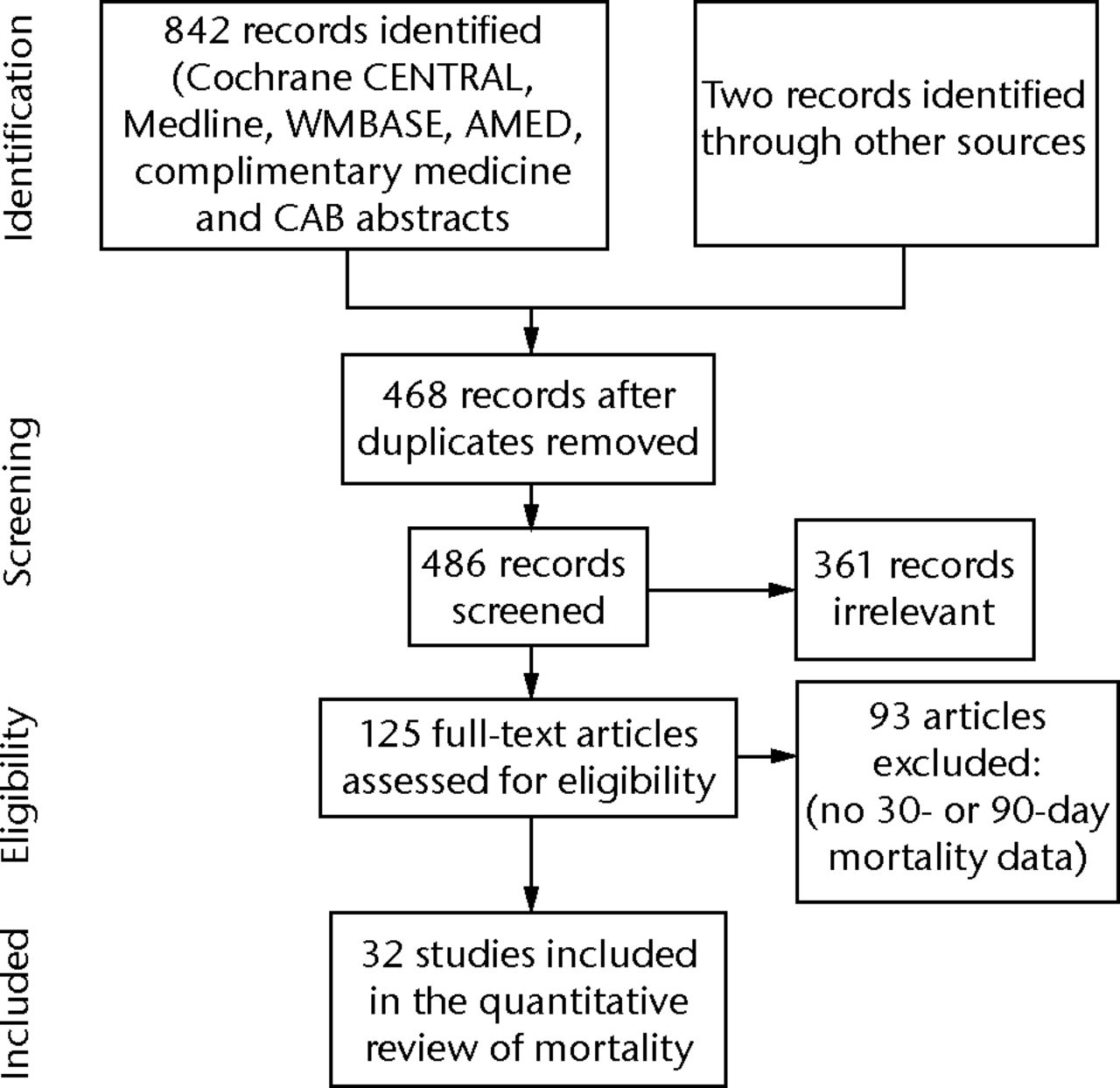
Fig. 1
Study flow diagram
Data extraction
The primary outcome was the incidence of mortality (either at 30 or 90 days post-operatively); and these data were extracted from the included studies. Study and participant characteristics were also recorded. In addition, we noted particular recurring themes of discussion, including the risk factors and common causes of mortality, and a summary is presented.
Statistical analysis
Because of the low prevalence of mortality in each study, the 95% confidence intervals were computed from a Poisson distribution. The pooled 30- and 90-day mortality rates were then estimated in meta-analyses.
Results
The 32 studies inform our estimate of post-operative mortality and include 1 129 330 patients.2,5-35 The largest contribution of data was from a UK study. It was published in 2013 and contained 409 096 patients.2 The smallest study contained 584 patients.11 In all, 10 studies report large (> 10 000 participants) cohorts, and of these, eight were studies of the national joint registries or national databases.2,5,7,16,17,21,22,35 A total of 18 studies were from the USA, one from Canada and 13 from European centres. A total of 19 of the 32 studies have been published in the last three years.
What is the overall early risk of mortality after hip replacement?
In view of the heterogeneity between studies (I2 93.0% and 98.2% for studies reporting 30- and 90-day mortality, respectively), and of the large number of potential risk factors for mortality influencing each study, we used a random effects model for our meta-analyses. These data were summarised in Figures 2 and 3.
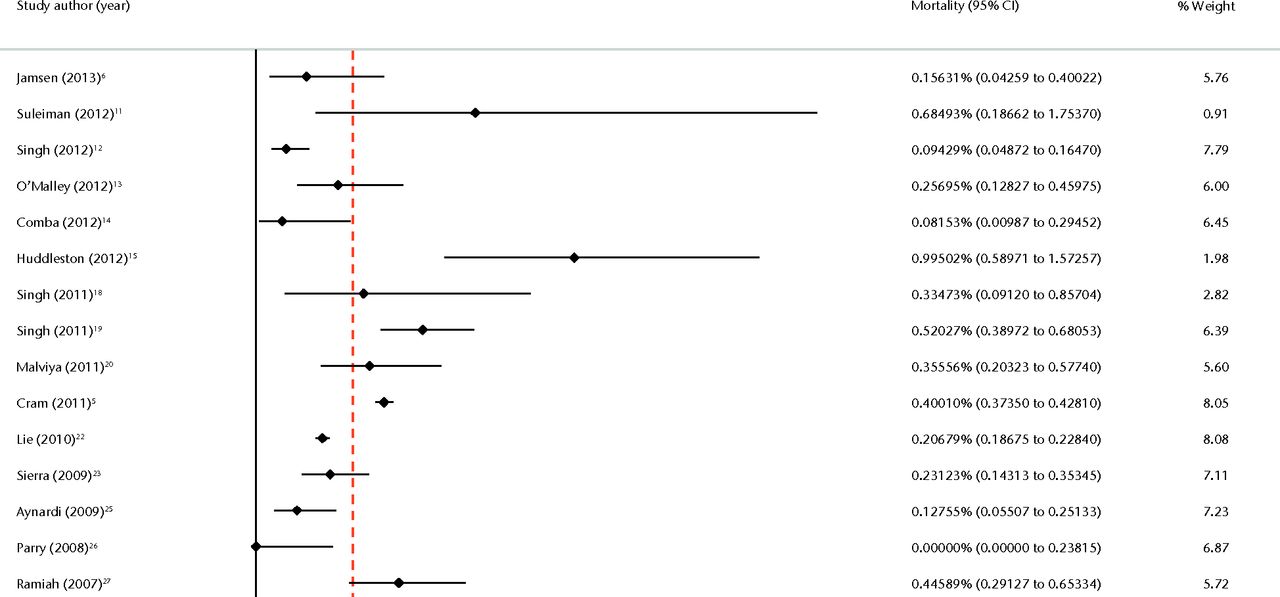
Fig. 2
Forest plot of 30-day mortality data.
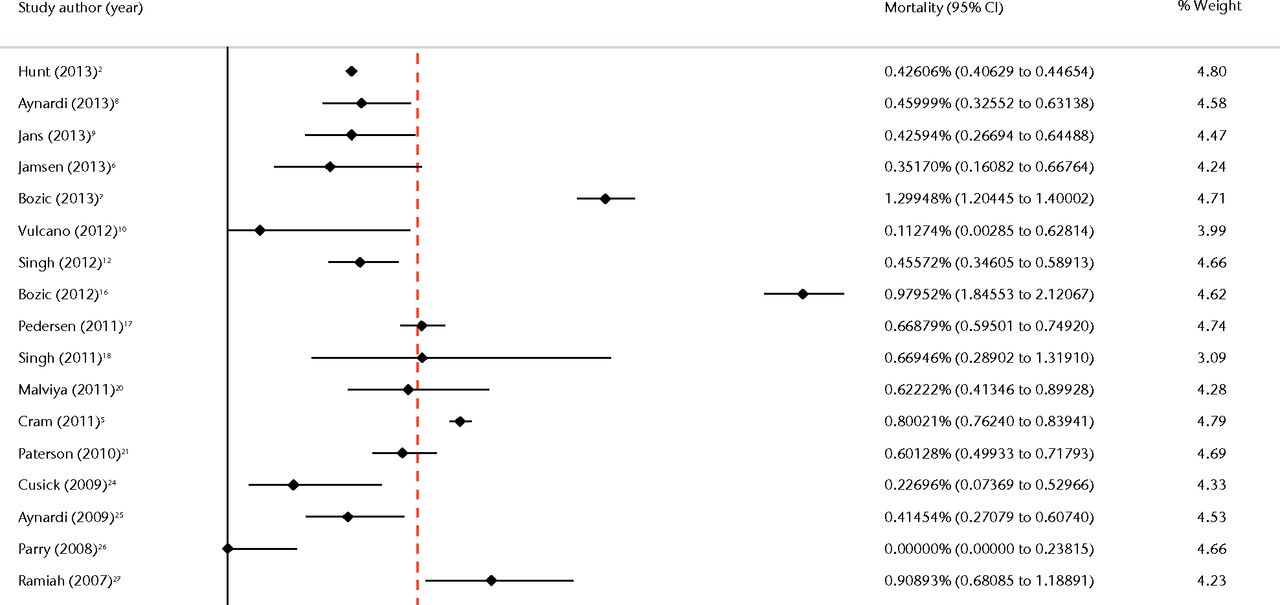
Fig. 3
Forest plot of 90-day mortality data.
Using data from the 32 studies in this review, the overall 30-day and 90-day mortality following THR was 0.30% (95% CI 0.22 to 0.38) and 0.65% (95% CI 0.50 to 0.81), respectively.
We performed sub-group analyses to identify the source of the heterogeneity. Study size, median year of data collection, geographical origin, and Medicare health insurance status were used to stratify the data in an attempt to identify the source. However, these subgroup analyses did not explain the heterogeneity. To contextualise the risk of mortality, we must compare it with that of a meaningful reference group. Studies providing standardised mortality ratios (SMRs) generally compare the observed mortality rate following THR with the expected mortality rate from an age- and sex-matched proportion of the general population not undergoing THR. Mahomed et al35 report a 90-day SMR of 0.9 (95% CI 0.8 to 1.0) during the 90 days following THR, indicating fewer deaths than expected.
In the search for an appropriate comparison group, Hochberg36 performed a systematic review of literature investigating mortality rates among patients with radiographically confirmed osteoarthritis. There was moderate evidence for an increased risk of death in patients with arthritis compared with the general population. However, weaknesses in the methodology of the studies on which this review is based, were acknowledged.
In the large population-based study of Nüesch et al,37 all-cause mortality was greater among patients with hip or knee arthritis compared with the general population: SMR 1.55 (95% CI 1.41 to 1.70). In particular, the incidence of cardiovascular-related mortality was high amongst patients with arthritis: SMR 1.71 (95% CI 1.49 to 1.98). In this study, SMRs were calculated using expected rates from whole population mortality data obtained via the Office for National Statistics (London, United Kingdom). A reduced capacity to exercise and the use of non-steroidal anti-inflammatory drugs in the arthritis group may partly explain these findings.
Due to perceived risks of surgery, the population selected for THR are likely to have a lower comorbidity score than the whole population of patients with arthritis. Parry et al26 attempt to address this potential for selection bias by comparing 30- and 90-day mortality rates, both between patients on the waiting list, and following total knee replacement surgery. Although this study was in knee replacement patients, it is noteworthy because of its methodology. Mortality was significantly greater in both the 30- and 90-day periods following surgery, compared with the same periods prior to surgery. The 30-day mortality was 0.0683% in the waiting list group and 0.37% following surgery (a five-fold increase). At 90 days, the mortality was 0.39% in the waiting list group and 0.79% following surgery.
The mortality rate in the waiting list group in this study was also lower than the SMR of the general population.26 This is known as the ‘well-patient effect,’ i.e. a selection bias towards well patients exists amongst those listed for surgery, who therefore benefit from an apparently reduced risk of mortality.38-40
This well-patient effect may also explain why numerous studies demonstrate improved long-term survival lasting up to 20 years following joint replacement surgery when compared with the matched general population.38-43 It is currently speculative to assume some health benefit is directly related to the procedure itself.
What temporal trends exist?
There is strong evidence to suggest that mortality rates following THR are decreasing. Hunt et al2 found a steady decrease in 90-day mortality from 0.56% in 2003, to 0.29% in 2011. These findings were based on a cohort of 409 096 patients with primary THRs from the National Joint Registry (NJR) for England and Wales,4 and are consistent with trends from a cohort of 1 453 493 Medicare patients in the USA.5 This study also showed a steady decline in 90-day mortality, from 1.2% in 1991 to 0.8% in 2008.5 The most recent Scottish Arthroplasty Project also reports the lowest 90-day mortality rates (< 0.5%) they have ever observed.44
Of the studies included in this review, four investigated the relationship between co-morbidity burden over time. All of these studies observed an increasing co-morbidity burden in patients undergoing THR.5,18,45,46 Reports were varied regarding the changing age demographic within primary THR. Two studies noted increasing age,5,18 and two report decreasing age.15,46 The mean age of the THR patient has, however, remained steady in the Scottish Arthroplasty Project,44 highlighting local differences in demographics and practice.
For how long is mortality risk elevated?
Barrett et al38 identified an increased risk of death immediately following surgery. They noted a crossing of survivorship curves before 90 days, when patients after THR were compared with an age and sex-matched population, including an attempt to control for comorbidities. Pedersen et al17 studied the Danish registry and identified a 30-day period of increased mortality immediately after THR surgery, but overall 90-day mortality was significantly lower than the age-, sex- and co-morbidity-matched general population (mortality rate ratio 0.8 (95% CI 0.7 to 0.9)).
In these studies, the cumulative risk of mortality must, by definition, lag behind the true daily risk. The study by Lie et al of 188 110 joint replacements in the Norwegian and Australian joint registries attempted to address this. They identified an excess mortality of 0.12% lasting for 26 days (95% CI 0.11% to 0.14%). After this period, daily mortality fell back to the baseline rates observed within the matched general population. The lack of adjustment for the well-patient effect in this study may artificially serve to reduce the observed period of increased risk.
In their analysis of the NJR for England and Wales, Hunt et al2 included a graph of smoothed Nelson–Aalen cumulative hazard estimates, which showed the changing risk of death over the first 90 post-operative days. The risk is highest in the first 30 days, and plateaus at around 90 days, suggesting that risk has returned to its baseline level in patients undergoing THR.
What are the common causes of mortality?
There appears to be a shift away from historical series such as that of Coventry et al47 in 1974, which quoted a mortality rate of 3% to 6% from pulmonary embolus alone.48 More recently, Blom et al49 reported a series of 1727 primary THRs performed with mechanical but no routine chemical thromboprophylaxis. Mortality within 90 days of surgery was 1%, however the risk of fatal pulmonary embolism within this time frame was 0.11%. Of the deaths that occurred in this series, ischaemic heart disease accounted for the majority (41.1%), followed by cerebrovascular accidents (23.1%), and pulmonary embolism (11.8%).49 Of the nine studies in this review reporting cause of mortality, eight identified cardiovascular causes (generally myocardial infarction or heart failure) as the leading cause of death,7-9,12,14,16,18,28 and in one small study, cerebrovascular accident was the leading cause of death.33 Cardiovascular disease is repeatedly cited as the leading cause of death following THR in modern series, followed by cerebrovascular disease or fatal pulmonary embolus.8,10,14,23,24,30,34,49-51 With longer follow-up, other causes such as malignancy, appear to become a significant cause of mortality.17
This pattern of mortality causation is reflected by the incidence of adverse events after THR. In the study by Singh et al,18 the incidence of cardiac complications was 6.9%, and thromboembolic complications 4.0%, within 90 days of THR
What are the risk factors for mortality?
Non-modifiable
There is strong evidence to suggest increasing age and male gender predispose to premature mortality following THR.2,6,12,21,22,34,25,52 In Blom et al’s study,49 risk of death was stratified by age. The 30-day mortality for the under 70 years age group was 0.00%, for the 70 to 79 year group it was 0.48%, and for the > 80 age group it was 1.43%.49 The association between increasing age and mortality following THR was consistent in the studies we identified. Although most studies also identified an association between male gender and increased mortality, two did not.8,28 The 30-day risk of mortality reported in the tenth (2013) Annual Report of the National Joint Registry for England, Wales and Northern Ireland ranges from 0.06% for woman aged < 55 years to 1.18% for men aged over 80 years.4
Modifiable patient factors
Several studies examined risk factors for mortality following THR by controlling for confounding variables using multivariate logistic regression analyses. The studies in this review found that an American Society of Anaesthesiologists risk score > 3,6,8,14 Charlson co-morbidity index > 3,8,12,16,21,35 use of general anaesthesia,2,8 and prior cardiovascular disease,9,12,14,16 were risk factors for mortality. Comba et al14 report that cardiovascular disease increased the risk of mortality eight-fold (odds ratio 8.83; 95% CI 1.78 to 43.6). Studies looking at earlier, peri-operative mortality, have identified pre-existing cardiovascular disease as a strong risk factor for early mortality after THR.52,53
Bozic et al16 performed a study using a multivariate cox regression analysis to identify hazard ratios (HR) for 90-day mortality using a 5% sample of the US Medicare population. Patients with metastatic cancer (HR 3.14), hemiplegia or paraplegia (HR 2.62), congestive heart failure (HR 2.11), dementia (HR 2.04), renal disease (HR1.98), psychosis (HR 1.85), cerebrovascular disease (HR 1.40), and chronic pulmonary disease (HR 1.32) were all statistically significantly associated with mortality up to 90 days.16 Hunt et al2 demonstrated a 10-fold increased risk for patients with moderate to severe liver disease, a three-fold increase following myocardial infarction and a two-fold increase following diabetes with complications and renal disease.2
Is body mass index (BMI) a risk factor for mortality after THR?
Data from Hunt et al’s2 analysis of the NJR for England and Wales showed that a BMI of 26 kg/m² to 30 kg/m² was associated with lower 90-day mortality, compared with patients with a normal BMI (defined as 19 kg/m² to 25 kg/m²; HR 0.76 (95% CI 0.62 to 0.92). This was consistent with the study of Jämsen et al,6 and although not statistically significant, the study of Bozic et al identified a trend towards reduced mortality in overweight patients.16
Huddleston found that obesity was associated with increased adverse events (p < 0.032), but did not identify a statistically significant association with mortality.15 Nüesch et al37 also found a protective effect of obesity on overall mortality in patients with osteoarthritis in univariate analysis, and although not statistically significant, the same trend was observed by multivariate analysis. The paradoxical protective effect of obesity on survival has been observed for other chronic conditions.54-57 This is known as the ‘obesity paradox.’ Whereas obesity itself is associated with an increased risk of developing conditions such as coronary artery disease or hypertension, once the condition is manifest, obesity protects against premature mortality when compared with non-obese patients.
Is the mortality after revision surgery comparable to primary hip replacement?
Aynardi et al25 reported mortality rates in a series of 7478 THRs, consisting of both primary and revision cases. The overall relative risk of mortality with revision THR was 1.24% at 90 days, compared with 0.41% following primary surgery. When stratified by age, with which the absolute risk of mortality for both primary and revision surgery increased, the relative mortality risk after revision compared with primary THR decreased within each age group.25 The study of Dearborn and Harris58 reported an overall post-operative mortality rate of 0.3% (eight deaths), with a rate of 0.2% (four deaths) after 2103 primary THRs and a rate of 0.6% (four deaths) after 633 revision THRs.58 Some studies did not report a difference, probably due to a lack of statistical power.52
Difference in mortality between hip and knee replacements
A total of seven studies reported unadjusted mortality data for THR and TKR.11,12,18,21,24,32,33 Six of these studies report a slightly higher mortality following THR. The overall difference in 30- and 90-day mortality rates following THR and TKR did not reach statistical significance (p = 0.30 and 0.30 respectively) (Table II and Table III).
Table II
Comparisons of 30-day mortality following total hip replacement (THR) and total knee replacement (TKR)
| 30-day mortality rate* | ||||||
|---|---|---|---|---|---|---|
| Author | Deaths (THR) | n (THR) | Incidence rate (THR) (%) | Deaths (TKR) | n (TKR) | Incidence rate (THR) (%) |
| Singh18 | 4 | 1195 | 0.335 | 4 | 1604 | 0.249 |
| Ibrahim32 | 48 | 6703 | 0.716 | 75 | 12108 | 0.619 |
| Suleiman11 | 4 | 584 | 0.685 | 3 | 1146 | 0.262 |
| Total | 56 | 8482 | 0.660 | 82 | 14858 | 0.552 |
-
*Z-Score 1.0383, p 0.29834
Table III
Comparisons of 90-day mortality following total hip replacement (THR) and total knee replacement (TKR)
| 90-day mortality rate* | ||||||
|---|---|---|---|---|---|---|
| Author | Deaths (THR) | n (THR) | Incidence rate (THR) (%) | Deaths (TKR) | n (TKR) | Incidence rate (THR) (%) |
| Singh12 | 58 | 12727 | 0.456 | 52 | 12484 | 0.417 |
| Singh18 | 8 | 1195 | 0.669 | 7 | 1604 | 0.436 |
| Paterson21 | 122 | 20290 | 0.601 | 144 | 27217 | 0.530 |
| Cusick24 | 5 | 2203 | 0.227 | 8 | 2050 | 0.390 |
| Vulcano10 | 1 | 887 | 0.113 | 2 | 645 | 0.310 |
| Nunley33 | 5 | 768 | 0.651 | 0 | 497 | 0 |
| Total | 199 | 38070 | 0.5325014 | 213 | 44497 | 0.4812 |
-
*Z-Score 1.276, p = 0.30302
Does hospital/surgeon volume influence mortality?
Some studies have suggested an association between low surgeon or hospital volume and increased mortality after THR.59-70 Many of these studies have been performed in the United States, where differences in the organisation of healthcare and individual surgical practices mean that these data may not be generalisable to practice in other settings. Singh et al19 studied death rates after THR in an American region according to hospital volume, using a multivariate analysis to control for age, gender, co-morbidity, insurance provider, and geographical region. Although no difference in 30-day mortality was identified between hospitals of varying volume, the largest volume units (> 200 THR/year) had the lowest one-year mortality. In the Canadian study of Paterson et al21, no relationship was identified between provider volume and mortality.
de Vries et al71 examined the association between unit procedure volume and complications after THR in a national study of all Dutch hospitals. Again, there was no significant association between volume and mortality. The lowest-volume group performed up to 100 THRs in a year, many more than low-volume groups used for comparison in other studies.
Chien et al72 examined surgeon procedure volume, observing a lower rate of adverse events and mortality after THR in patients treated by surgeons who performed > 25 procedures per year when compared with surgeons performing < 10 per year (mortality rates 0.57% and 2.55% respectively, adjusted OR 0.23).
After examining the studies in this review, it is difficult to make any firm conclusion regarding the effect of surgeon or unit volume on mortality. Local differences in training, healthcare organisation, and the extremes of case volume may account for observed differences.
Limitations
When interpreting data on mortality following joint replacement, selection bias remains a key confounder. Multivariate analyses can only control for the confounding data that have been collected, and cannot eliminate all aspects of bias. Studies including hip fracture patients, revision hip replacement patients, high numbers of patients with state-funded Medicare insurance, particular co-morbidities, or extremes of age, may explain the variation among reported mortality rates. For example, in studies which compare this subset of the population with the privately funded population undergoing THR, a higher mortality is noted amongst the Medicare population.73 The complex relationship between socioeconomic status and outcomes following THR has been studied by Clement et al.74 They identified an association between deprivation and outcomes such as dislocation and 90-day mortality.
Conclusion
THR is associated with a small increase in the risk of mortality in the immediate post-operative period, however, this risk appears to be reducing every year. The majority of excess mortality risk occurs in the first 30 days and has returned to baseline by 90 days. This reduction in mortality over time may be multifactorial, and is partially explained by the secular decline in mortality that has led to our ageing population. The introduction of the multi-disciplinary pre-operative assessment clinic has been shown to reduce mortality following joint replacement.75 Length of hospital stay also appears to be reducing,45 and the incidence of serious adverse events is decreasing.15 In addition, there has been a shift towards practices, such as spinal anaesthetic and routine thromboprophylaxis, that are associated with lower mortality.2
In recent years, improved surgical safety and better post-operative care appear to have brought about a reduction in mortality following THR. Mortality will continue to change, affected by medical advancements, social factors and the organisation of health care as it continues to develop. It is likely that the trend for reduced mortality after THR will continue. Data presented here allow patients to make informed choices and allow clinicians to address modifiable surgeon and patient factors that contribute to mortality.
1 Learmonth ID , YoungC, RorabeckC. The operation of the century: total hip replacement. Lancet2007;370:1508–1519.CrossrefPubMed Google Scholar
2 Hunt LP , Ben-ShlomoY, ClarkEM, et al.90-day mortality after 409,096 total hip replacements for osteoarthritis, from the National Joint Registry for England and Wales: a retrospective analysis. Lancet2013;382:1097–1104.CrossrefPubMed Google Scholar
3 Stroup DF , BerlinJA, MortonSC, et al.Meta-analysis of observational studies in epidemiology: a proposal for reporting. Meta-analysis Of Observational Studies in Epidemiology (MOOSE) group. JAMA2000;283:2008–2012.CrossrefPubMed Google Scholar
4 No authors listed. National Joint Registry for England and Wales 10th Annual Report 2013. http://www.njrcentre.org.uk/njrcentre/Portals/0/Documents/England/Reports/10th_annual_report/NJR%2010th%20Annual%20Report%202013.pdf. (date last accessed 1 October 2013). Google Scholar
5 Cram P , LuX, KaboliPJ, et al.Clinical characteristics and outcomes of Medicare patients undergoing total hip arthroplasty, 1991-2008. JAMA2011;305:1560–1567.CrossrefPubMed Google Scholar
6 Jämsen E , PuolakkaT, EskelinenA, et al.Predictors of mortality following primary hip and knee replacement in the aged. A single-center analysis of 1,998 primary hip and knee replacements for primary osteoarthritis. Acta Orthop2013;84:44–53.CrossrefPubMed Google Scholar
7 Bozic KJ , OngK, LauE, et al.Estimating risk in Medicare patients with THA: an electronic risk calculator for periprosthetic joint infection and mortality hip. Clin Orthop Relat Res2013;471:574–583. Google Scholar
8 Aynardi M , JacovidesCL, HuangR, MortazaviSM, ParviziJ. Risk factors for early mortality following modern total hip arthroplasty. J Arthroplasty2013;28:517–520.CrossrefPubMed Google Scholar
9 Jans O, Jorgensen C, Kehlet H, Johansson PI, Lundbeck Foundation Centre for Fast-track Hip and Knee Replacement Collaborative Group. Role of preoperative anemia for risk of transfusion and postoperative morbidity in fast-track hip and knee arthroplasty Transfusion2014;54:717–726. Google Scholar
10 Vulcano E , GesellM, EspositoA, et al.Aspirin for elective hip and knee arthroplasty: A multimodal thromboprophylaxis protocol. Int Orthop2012;36:1995–2002.CrossrefPubMed Google Scholar
11 Suleiman LI , OrtegaG, Ong UtiSK, et al.Does BMI affect perioperative complications following total knee and hip arthroplasty?J Surg Res2012;174:7–11.CrossrefPubMed Google Scholar
12 Singh JA, Lewallen DG. Ninety-day mortality in patients undergoing elective total hip or total knee arthroplasty. J Arthroplasty 2012;27:1417-22 e1. Google Scholar
13 O’Malley NT , FlemingFJ, GunzlerDD, MessingSP, KatesSL. Factors Independently Associated With Complications and Length of Stay after Hip Arthroplasty. Analysis of the National Surgical Quality Improvement Program. J Arthroplasty2012;27:1832–1837. Google Scholar
14 Comba F , Alonso-HidalgoI, ButtaroM, PiccalugaF. Risk Factor Analysis for 30-Day Mortality After Primary THA in a Single Institution. HSS J 2012;8:111–115.CrossrefPubMed Google Scholar
15 Huddleston JI , WangY, UquillasC, HerndonJH, MaloneyWJ. Age and obesity are risk factors for adverse events after total hip arthroplasty. Clin Orthop Relat Res2012;470:490–496.CrossrefPubMed Google Scholar
16 Bozic KJ , LauE, KurtzS, et al.Patient-related risk factors for periprosthetic joint infection and postoperative mortality following total hip arthroplasty in Medicare patients. J Bone Joint Surg [Am]2012;94-A:794–800.CrossrefPubMed Google Scholar
17 Pedersen AB , BaronJA, OvergaardS, JohnsenSP. Short- and long-term mortality following primary total hip replacement for osteoarthritis: a Danish nationwide epidemiological study. J Bone Joint Surg [Br]2011;93-B:172–177.CrossrefPubMed Google Scholar
18 Singh JA , JensenMR, HarmsenWS, GabrielSE, LewallenDG. Cardiac and thromboembolic complications and mortality in patients undergoing total hip and total knee arthroplasty. Ann Rheum Dis2011;70:2082–2088.CrossrefPubMed Google Scholar
19 Singh JA , KwohCK, BoudreauRM, LeeGC, IbrahimSA. Hospital volume and surgical outcomes after elective hip/knee arthroplasty: A risk-adjusted analysis of a large regional database. Arthritis Rheum2011;63:2531–2539.CrossrefPubMed Google Scholar
20 Malviya A , MartinK, HarperI, et al.Enhanced recovery program for hip and knee replacement reduces death rate. Acta Orthopaedica2011;82:577–581.CrossrefPubMed Google Scholar
21 Paterson JM , WilliamsJI, KrederHJ, et al.Provider volumes and early outcomes of primary total joint replacement in Ontario. Can J Surg2010;53:175–183.PubMed Google Scholar
22 Lie SA , PrattN, RyanP, et al.Duration of the increase in early postoperative mortality after elective hip and knee replacement. J Bone Joint Surg [Am]2010;92-A:58–63.CrossrefPubMed Google Scholar
23 Sierra RJ , TimperleyJA, GieGA. Contemporary Cementing Technique and Mortality During and After Exeter Total Hip Arthroplasty. J Arthroplasty2009;24:325–332.CrossrefPubMed Google Scholar
24 Cusick LA , BeverlandDE. The incidence of fatal pulmonary embolism after primary hip and knee replacement in a consecutive series of 4253 patients. J Bone Joint Surg [Br]2009;91-B:645–648.CrossrefPubMed Google Scholar
25 Aynardi M , PulidoL, ParviziJ, SharkeyPF, RothmanRH. Early mortality after modern total hip arthroplasty. Clin Orthop Relat Res2009;467:213–218.CrossrefPubMed Google Scholar
26 Parry M , WyldeV, BlomAW. Ninety-day mortality after elective total hip replacement: 1549 patients using aspirin as a thromboprophylactic agent. J Bone Joint Surg [Br]2008;90-B:306–307.CrossrefPubMed Google Scholar
27 Ramiah RD , AshmoreAM, WhitleyE, BannisterGC. Ten-year life expectancy after primary total hip replacement. J Bone Joint Surg [Br]2007;89-B:1299–1302.CrossrefPubMed Google Scholar
28 Gaston MS , AminAK, ClaytonRA, BrenkelIJ. Does a history of cardiac disease or hypertension increase mortality following primary elective total hip arthroplasty?Surgeon2007;5:260–265. Google Scholar
29 Samama CM , RavaudP, ParentF, et al.Epidemiology of venous thromboembolism after lower limb arthroplasty: the FOTO study. J Thromb Haemost2007;5:2360–2367.CrossrefPubMed Google Scholar
30 Tarity TD , HerzAL, ParviziJ, RothmanRH. Ninety-Day Mortality After Hip Arthroplasty. A Comparison Between Unilateral and Simultaneous Bilateral Procedures. J Arthroplasty2006;21(suppl):60–64. Google Scholar
31 Blom A , PattisonG, WhitehouseS, TaylorA, BannisterG. Early death following primary total hip arthroplasty: 1,727 procedures with mechanical thrombo-prophylaxis. Acta Orthop2006;77:347–350.CrossrefPubMed Google Scholar
32 Ibrahim SA , StoneRA, HanX, et al.Racial/ethnic differences in surgical outcomes in veterans following knee or hip arthroplasty. Arthritis Rheum2005;52:3143–3151. Google Scholar
33 Nunley RM , LachiewiczPF. Mortality after total hip and knee arthroplasty in a medium-volume university practice. J Arthroplasty2003;18:278–285.CrossrefPubMed Google Scholar
34 Miller KA , CallaghanJJ, GoetzDD, JohnstonRC. Early postoperative mortality following total hip arthroplasty in a community setting: a single surgeon experience. Iowa Orthop J2003;23:36–42.PubMed Google Scholar
35 Mahomed NN , BarrettJA, KatzJN, et al.Rates and outcomes of primary and revision total hip replacement in the United States medicare population. J Bone Joint Surg [Am]2003;85-A:27–32.CrossrefPubMed Google Scholar
36 Hochberg MC. Mortality in osteoarthritis. Clin Exp Rheumatol 2008;26(Suppl 51)S:120–124. Google Scholar
37 Nüesch E , DieppeP, ReichenbachS, et al.All cause and disease specific mortality in patients with knee or hip osteoarthritis: population based cohort study. BMJ2011;342:1165. Google Scholar
38 Barrett J , LosinaE, BaronJA, et al.Survival following total hip replacement. J Bone Joint Surg [Am]2005;87-A:1965–1971.CrossrefPubMed Google Scholar
39 Lie SA , EngesaeterLB, HavelinLI, GjessingHK, VollsetSE. Mortality after total hip replacement: 0-10-year follow-up of 39,543 patients in the Norwegian Arthroplasty Register. Acta Orthop Scand2000;71:19–27.CrossrefPubMed Google Scholar
40 Holmberg S . Life expectancy after total hip arthroplasty. J Arthroplasty1992;7:183–186.CrossrefPubMed Google Scholar
41 Schroder HM , KristensenPW, PetersenMB, NielsenPT. Patient survival after total knee arthroplasty. 5-year data in 926 patients. Acta Orthop Scand1998;69:35–38.CrossrefPubMed Google Scholar
42 Visuri T , PulkkinenP, TurulaKB, PaavolainenP, KoskenvuoM. Life expectancy after hip arthroplasty. Case-control study of 1018 cases of primary arthrosis. Acta Orthop Scand1994;65:9–11.CrossrefPubMed Google Scholar
43 Visuri T , BorgH, PulkkinenP, PaavolainenP, PukkalaE. A retrospective comparative study of mortality and causes of death among patients with metal-on-metal and metal-on-polyethylene total hip prostheses in primary osteoarthritis after a long-term follow-up. BMC Musculoskelet Disord2010;11:78.CrossrefPubMed Google Scholar
44 No authors listed. Scottish Arthroplasty Project Biennial Report 2012. http://www.arthro.scot.nhs.uk/ (last accessed 27 Sept 2013). Google Scholar
45 Jimenez-Garcia R , Villanueva-MartinezM, Fernandez-de-Las-PenasC, et al.Trends in primary total hip arthroplasty in Spain from 2001 to 2008: evaluating changes in demographics, comorbidity, incidence rates, length of stay, costs and mortality. BMC Musculoskelet Disord2011;12:43.CrossrefPubMed Google Scholar
46 Kirksey M , ChiuYL, MaY, et al.Trends in in-hospital major morbidity and mortality after total joint arthroplasty: United States 1998-2008. Anesth Analg2012;115:321–327.CrossrefPubMed Google Scholar
47 Coventry MB , BeckenbaughRD, NolanDR, IlstrupDM. 2,012 total hip arthroplasties. A study of postoperative course and early complications. J Bone Joint Surg [Am]1974;56-A:273–284.PubMed Google Scholar
48 Johnson R , GreenJR, CharnleyJ. Pulmonary embolism and its prophylaxis following the Charnley total hip replacement. Clin Orthop Relat Res1977;127:123–132.PubMed Google Scholar
49 Blom A , PattisonG, WhitehouseS, TaylorA, BannisterG. Early death following primary total hip arthroplasty: 1,727 Procedures with mechanical thrombo-prophylaxis. Acta Orthop2006;77:347–350.CrossrefPubMed Google Scholar
50 Poultsides LA , Gonzalez Della ValleA, MemtsoudisSG, et al.Meta-analysis of cause of death following total joint replacement using different thromboprophylaxis regimens. J Bone Joint Surg [Br]2012;94-B:113–121.CrossrefPubMed Google Scholar
51 Paavolainen P , PukkalaE, PulkkinenP, VisuriT. Causes of death after total hip arthroplasty: a nationwide cohort study with 24,638 patients. J Arthroplasty2002;17:274–281.CrossrefPubMed Google Scholar
52 Parvizi J , JohnsonBG, RowlandC, ErethMH, LewallenDG. Thirty-day mortality after elective total hip arthroplasty. J Bone Joint Surg [Am]2001;83-A:1524–1528.CrossrefPubMed Google Scholar
53 Memtsoudis SG , PumbergerM, MaY, et al.Epidemiology and risk factors for perioperative mortality after total hip and knee arthroplasty. J Orthop Res2012;30:1811–1821.CrossrefPubMed Google Scholar
54 Haass M , KitzmanDW, AnandIS, et al.Body mass index and adverse cardiovascular outcomes in heart failure patients with preserved ejection fraction: results from the Irbesartan in Heart Failure with Preserved Ejection Fraction (I-PRESERVE) trial. Circ Heart Fail2011;4:324–331.CrossrefPubMed Google Scholar
55 Curtis JP , SelterJG, WangY, et al.The obesity paradox: body mass index and outcomes in patients with heart failure. Arch Intern Med2005;165:55–61.CrossrefPubMed Google Scholar
56 Bakaeen FG, Chu D. The obesity paradox and cardiac surgery: are we sending the wrong message? Ann Thorac Surg 2011;92-4:1153. Google Scholar
57 Stamou SC , NussbaumM, StiegelRM, et al.Effect of body mass index on outcomes after cardiac surgery: is there an obesity paradox?Ann Thorac Surg2011;91:42–47.CrossrefPubMed Google Scholar
58 Dearborn JT , HarrisWH. Postoperative mortality after total hip arthroplasty. An analysis of deaths after two thousand seven hundred and thirty-six procedures. J Bone Joint Surg [Am]1998;80-A:1291–1294.CrossrefPubMed Google Scholar
59 Kreder HJ , DeyoRA, KoepsellT, SwiontkowskiMF, KreuterW. Relationship between the volume of total hip replacements performed by providers and the rates of postoperative complications in the state of Washington. J Bone Joint Surg [Am]1997;79-A:485–494.PubMed Google Scholar
60 Katz JN , LosinaE, BarrettJ, et al.Association between hospital and surgeon procedure volume and outcomes of total hip replacement in the United States Medicare population. J Bone Joint Surg [Am]2001;83-A:1622–1629.CrossrefPubMed Google Scholar
61 Solomon DH , LosinaE, BaronJA, et al.Contribution of hospital characteristics to the volume-outcome relationship – dislocation and infection following total hip replacement surgery. Arthritis Rheum2002;46:2436–2444. Google Scholar
62 Losina E , BarrettJ, MahomedNN, BaronJA, KatzJN. Early failures of total hip replacement: effects of surgeon volume. Arthritis Rheum2004;50:1338–1343. Google Scholar
63 Battaglia TC , MulhallKJ, BrownTE, SalehKJ. Increased surgical volume is associated with lower THA dislocation rates. Clin Orthop Relat Res2006;447:28–33.CrossrefPubMed Google Scholar
64 Doro C , DimickJ, WainessR, UpchurchG, UrquhartA. Hospital Volume and Inpatient Mortality Outcomes of Total Hip Arthroplasty in the United States. J Arthroplasty2006;21(Suppl):10–16.CrossrefPubMed Google Scholar
65 Judge A , ChardJ, LearmonthI, DieppeP. The effects of surgical volumes and training centre status on outcomes following total joint replacement: Analysis of the Hospital Episode Statistics for England. J Public Health2006;28:116–124.CrossrefPubMed Google Scholar
66 Cram P , Vaughan-SarrazinMS, WolfB, KatzJN, RosenthalGE. A comparison of total hip and knee replacement in specialty and general hospitals. J Bone Joint Surg [Am]2007;89-A:1675–1684.CrossrefPubMed Google Scholar
67 Shervin N , RubashHE, KatzJN. Orthopaedic procedure volume and patient outcomes: a systematic literature review. Clin Orthop Relat Res2007;457:35–41.CrossrefPubMed Google Scholar
68 SooHoo NF , FarngE, LiebermanJR, ChambersL, ZingmondDS. Factors That Predict Short-term Complication Rates After Total Hip Arthroplasty. Clin Orthop Relat Res2010;468:2363–2371.CrossrefPubMed Google Scholar
69 Manley M , OngK, LauE, KurtzSM. Effect of Volume on Total Hip Arthroplasty Revision Rates in the United States Medicare Population. J Bone Joint Surg [Am]2008;90-A:2446–2451.CrossrefPubMed Google Scholar
70 Bozic KJ , MaselliJ, PekowPS, et al.The Influence of Procedure Volumes and Standardization of Care on Quality and Efficiency in Total Joint Replacement Surgery. J Bone Joint Surg [Am]2010;92-A:2643–2652.CrossrefPubMed Google Scholar
71 de Vries LM , SturkenboomMC, VerhaarJA, KingmaJH, StrickerBH. Complications after hip arthroplasty and the association with hospital procedure volume: a nationwide retrospective cohort study on 50,080 total hip replacements with a follow-up of 3 months after surgery. Acta Orthop2011;82:545–552. Google Scholar
72 Chien LN , ChuHF, LiuCH, et al.Association between hospital and surgeon procedure volume with outcome of total hip replacement. [Article in Chinese]. Taiwan Journal of Public Health2003;22:118–126. Google Scholar
73 Memtsoudis SG , Gonzalez Della ValleA, BesculidesMC, et al.Risk factors for perioperative mortality after lower extremity arthroplasty: a population-based study of 6,901,324 patient discharges. J Arthroplasty2010;25:19–26.CrossrefPubMed Google Scholar
74 Clement ND , MuzammilA, MacDonaldD, HowieCR, BiantLC. Socioeconomic status affects the early outcome of total hip replacement. J Bone Joint Surg [Br]2011;93-B:464–469.CrossrefPubMed Google Scholar
75 Kamal T , ConwayRM, LittlejohnI, RickettsD. The role of a multidisciplinary pre-assessment clinic in reducing mortality after complex orthopaedic surgery. An R Coll Surg Eng2011;93:149–151.CrossrefPubMed Google Scholar
Funding statement:
None declared
Author contributions:
J. R. Berstock: Literature search, Data extraction, Writing the paper
A. D. Beswick: Literature search, Data extraction, Writing the paper
E. Lenguerrand: Statistical/data analysis
M. R. Whitehouse: Revision of manuscript
A. W. Blom: Revision of manuscript
ICMJE Conflict of Interest:
None declared
©2014 The British Editorial Society of Bone & Joint Surgery. This is an open-access article distributed under the terms of the Creative Commons Attributions licence, which permits unrestricted use, distribution, and reproduction in any medium, but not for commercial gain, provided the original author and source are credited.
Supplementary material. Two tables showing reported mortality and study characteristics are available with the electronic version of this article on our website at www.jbjs.org.uk
