





Abstract
Objectives
Our study aimed to examine if a mobile-bearing total knee replacement (TKR) offered an advantage over fixed-bearing designs with respect to rates of secondary resurfacing of the patella in knees in which it was initially left unresurfaced.
Methods
We examined the 11-year report of the New Zealand Joint Registry and identified all primary TKR designs that had been implanted in > 500 knees without primary resurfacing of the patella. We examined how many of these were mobile-bearing, fixed-bearing cruciate-retaining and fixed-bearing posterior-stabilised designs. We assessed the rates of secondary resurfacing of the patella for each group and constructed Kaplan-Meier survival curves.
Results
Our study showed a significantly higher rate of revision for secondary resurfacing of the patella in the fixed-bearing posterior-stabilised TKR designs compared with either fixed-bearing cruciate-retaining or mobile-bearing designs (p = 0.001 and p = 0.036, respectively).
Conclusions
This New Zealand Registry study shows that during the last 11 years, revision procedures to resurface an unresurfaced patella in primary TKR occurred at a higher rate in fixed-bearing posterior-stabilised designs.
Article focus
To investigate total knee replacements (TKRs) undertaken for osteoarthritis
To assess whether mobile- or fixed-bearing TKRs were protective of an un-resurfaced patella in terms of secondary resurfacing of the patella in modern TKR designs
Key messages
New Zealand Joint Registry Study focused on TKRs implanted in numbers > 500 knees in the 11-year report
Stratification of TKRs into mobile-bearing, fixed-bearing cruciate-retaining and fixed-bearing posterior-stabilised designs, all performed without resurfacing of the patella at primary operation
Comparison of rates of secondary resurfacing of the patella between the bearing groups
Strengths and limitations
A total of 20 495 primary TKRs implanted without initial patellar resurfacing, with 96% follow-up
We assumed that all secondary resurfacings patellar were undertaken for pain, with a constant surgeon intervention rate
There were no details in the registry regarding circumferential patella electrocautery and its effect on rates of revision
Introduction
There is a rapidly increasing demand for total knee replacement (TKR) worldwide and the role of resurfacing of the patella remains an important question. There are currently profound geographical differences regarding resurfacing in the osteo-arthritic knee: in the New Zealand Joint Registry the majority of TKRs have the patella un-resurfaced1 while several studies from the Unites States show the opposite.2-5 There are conflicting results from Level 1 studies on whether or not to resurface the patella at the time of primary TKR for osteoarthritis. Some surgeons may consider it necessary in selected cases, such as in the rheumatoid knee.6 Waters and Bentley7 performed a prospective randomised controlled trial of patellar resurfacing in 514 cruciate-retaining (CR) and posterior-stabilised (PS) TKRs, and found a higher rate of revision for patellofemoral pain in those knees in which resurfacing had not been performed. Conversely, Burnett et al8 undertook a prospective randomised controlled trial of 100 CR TKRs in 90 patients for a minimum of ten years. They found no significant differences in functional score, satisfaction, anterior knee pain or rate of revision between knees that had undergone resurfacing of the patella and those that had not.8 The authors therefore did not advocate patellar resurfacing.
There is also evidence that the functional results after secondary patellar resurfacing for pain after primary TKR are not only less predictable but also less favourable than if the patella was resurfaced at the index procedure.9,10
Mobile-bearing TKRs are potentially more ‘patella-friendly’ from a biomechanical standpoint, as they may provide more forgiving tibiofemoral kinematics. A prospective randomised controlled trial of bilateral LCS mobile-bearing TKRs (DePuy Orthopaedics Inc., Warsaw, Indiana), with one patella resurfaced and the other not, showed that the mobile bearing did not convey an additional advantage over leaving the patella unresurfaced,11 and this also supports findings from the Swedish Joint Registry.12
Materials and Methods
The aim of this study was to compare the rates of a second operation to resurface the patella after a primary TKR for osteoarthritis using a PS, CR or mobile-bearing modern TKR designs used in New Zealand.
The New Zealand Joint Registry has over 11 years of prospective data and a 96% capture rate. Since its inception after ethical approval in 1998, over 38 326 primary TKRs have been performed, 70% of which did not have the patella resurfaced.
We used the 11-year report1 to identify TKR designs implanted in > 500 knees. We then obtained the product numbers from the Registry and classified these implants as fixed- or mobile-bearing implants. We did not differentiate the mobile-bearing group as to whether PS or CR. We stratified the fixed-bearing TKRs into CR and PS designs and identified how many of each group had the patella resurfaced at index surgery. We then examined the Registry data for rates of revision for patellar resurfacing.
Statistical analysis
The data were analysed by a medical statistician (CF) with 95% confidence intervals calculated and significance testing performed using Student’s t-test (SPSS v19; SPSS Inc., Chicago, Illinois). A p-value < 0.05 was considered to denote statistical significance.
Results
From the 11-year report (January 1999 and December 2009) of the New Zealand Joint Registry we identified 20 945 TKRs implanted for osteoarthritis, which had not had the patella resurfaced. Only implants with > 500 were included. The numbers of fixed-bearing CR, fixed-bearing PS and mobile-bearing implants and their revision rates for secondary resurfacing of the patella are shown in Table I.
Table I
Rates of revision for secondary patellar resurfacing in fixed-bearing (FB) cruciate-retaining (CR), FB posterior-stabilised (PS) and mobile-bearing (MB) total knee replacements implanted in numbers > 500 in New Zealand (CI, confidence interval)
| Design | p-values | ||||||
|---|---|---|---|---|---|---|---|
| FB CR | FB PS | MB | FB CR vs FB PS | FB CR vs MB | FB PS vs MB | ||
| Knees without primary patellar resurfacing (n) | 13 595 | 3852 | 3518 | ||||
| Secondary patellar resurfacing (n) | 81 | 39 | 21 | ||||
| Rate of revision per 100 component years (%) (95% CI) | 0.14 (0.12 to 0.18) | 0.29 (0.2 to 0.39) | 0.16 (0.1 to 0.25) | 0.001 | 0.863 | 0.036 | |
These results were used to construct a Kaplan-Meier survival curve (Fig. 1). CR fixed-bearing TKRs had the lowest rate of secondary patellar resurfacing but not significantly greater than mobile-bearing (p = 0.863). PS fixed-bearing TKRs had a significantly greater rate of secondary patellar resurfacing compared with both mobile-bearing (p = 0.036) and CR fixed-bearing TKRs (p = 0.001) in the New Zealand Joint Registry.
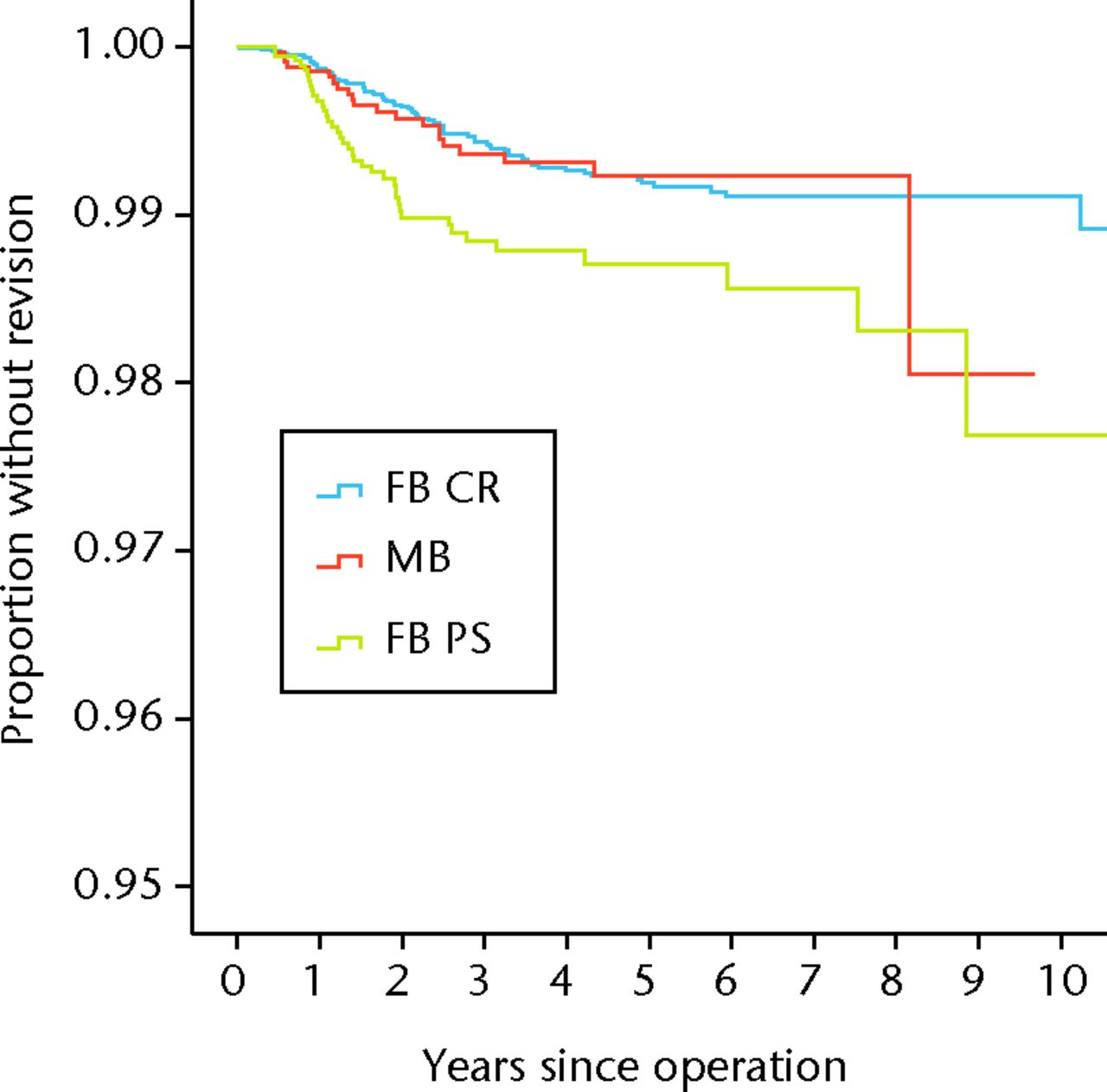
Fig. 1
Kaplan-Meier survival curve of fixed-bearing (FB) cruciate-retaining (CR), FB posterior-stabilised (PS) and mobile-bearing (MB) total knee replacements, with secondary patellar resurfacing as the endpoint.
Discussion
This New Zealand Joint Registry study of modern TKR designs suggests that CR fixed-bearing and mobile-bearing TKR designs implanted without resurfacing of the patella are superior to fixed-bearing PS designs in terms of rates of secondary patellar resurfacing. Within each group there were several different manufactures and therefore designs, but it was not possible to analyse each subset within the broad grouping as the numbers would not have been sufficient to have produced a statistically significant result. These results agree with the prospective randomised controlled trial using CR fixed-bearing protheses by Burnett et al.8 In addition our results are consistent with the findings of Keblish et al,12 and imply that the patella can be left unresurfaced if using a mobile-bearing design. Our results suggest that the use of a fixed-bearing PS TKR may be an indication for resurfacing of the patella at the index procedure. However, a therapeutic trial would ideally be performed to determine true clinical significance. We propose that this finding may be because the PS design leads to increased stresses at the patellofemoral joint compared with the mobile-bearing or CR designs.
This study has several weaknesses. It is a retrospective review of Registry data and does not record the indication for secondary resurfacing of the patella, nor the surgeon’s practice of using electrocautery around the unresurfaced patella – there is evidence that such treatment may improve post-operative pain.13 We have assumed that modern patellar resurfacings and TKR designs are very similar in terms of their functional results. For simplicity, and directly as a result of what data is recorded in the New Zealand Joint Registry, we have assumed that secondary resurfacing in our study was performed for anterior knee pain rather than instability. In addition there is a paucity of knowledge as to why patients develop anterior knee pain when the patella is left un-resurfaced. This study does not support the view that mobile-bearing TKR designs are more ‘patella-friendly’ than PS or CR fixed-bearing designs.
1 New Zealand Joint Registry. Thirteen year report, 2011. http://www.cdhb.govt.nz/njr/reports/A2D65CA3.pdf (date last accessed 28 June 2013). Google Scholar
2 Schindler OS . The controversy of patellar resurfacing in total knee arthroplasty: Ibisne in medio tutissimus?Knee Surg Traumatol Arthrosc2012;20:1227–1244.CrossrefPubMed Google Scholar
3 Burnett RS , BourneRB. Indications for patellar resurfacing in total knee arthroplasty. Instr Course Lect.2004;53:167–186.PubMed Google Scholar
4 Meneghini RM . Should the patella be resurfaced in primary total knee arthroplasty?: an evidence-based analysis. J Arthroplasty2008;23(Suppl):11–14. Google Scholar
5 Johnson TC , TatmanPJ, MehleS, GloeTJ. Revision surgery for patellofemoral problems: should we always resurface?Clin Orthop Relat Res2012;470:211–219.CrossrefPubMed Google Scholar
6 Swan JD , StoneyJS, LimK, DowseyMM, ChoongPF. The need for patellar resurfacing in total knee arthroplasty: a literature review. ANZ J Surg2010;80:223–233.CrossrefPubMed Google Scholar
7 Waters TS , BentleyG. Patella resurfacing in total knee arthroplasty: a prospective, randomized study. J Bone Joint Surg [Am]2003;85-A:212–217. Google Scholar
8 Burnett RS , BooneJL, McCarthyKP, RosenzweigS, BarrackRL. A prospective randomized clinical trial of patellar resurfacing and nonresurfacing in bilateral TKA. Clin Orthop Relat Res2007;464:65–72.CrossrefPubMed Google Scholar
9 Lygre SH , EspehaugB, HavelinLI, VollsetSE, FurnesO. Failure of total knee replacement with or without patella resurfacing patellar resurfacing. Acta Orthop2011;82:282–292. Google Scholar
10 Mockford BJ , BeverlandDE. Secondary resurfacing of the patella in mobile-bearing total knee arthroplasty. J Arthroplasty2005;20:898–902.CrossrefPubMed Google Scholar
11 Sawaguchi N , MajimaT, IshigakiTJ, et al.Mobile-bearing total knee arthroplasty improves patellar tracking and patellofemoral contact stress: in vivo measurements in the same patients. J Arthroplasty2010;25:920–925.CrossrefPubMed Google Scholar
12 Keblish PA , VarmaAK, GreenwaldAS. Patella resurfacing or retention in total knee arthroplasty: a prospective study of patients with bilateral replacements. J Bone Joint Surg [Br]1994;76-B:930–937. Google Scholar
13 van Jonbergen HPW , ScholtesVAB, van KampenA, PoolmanRW. A randomized, controlled trial of circumpatellar electrocautery in total knee replacement without patella resurfacing. J Bone Joint Surg [Br]2011;93-B:1054–1059. Google Scholar
Funding statement:
No funding was received in support of this study
Author contributions:
M. C. Wyatt: Writing the paper
C. Frampton: Data collation, Statistical analysis, Manuscript review
J. G. Horne: Writing the paper
P. Devane: Manuscript review
ICMJE Conflict of Interest:
None declared
©2013 The British Editorial Society of Bone & Joint Surgery. This is an open-access article distributed under the terms of the Creative Commons Attributions licence, which permits unrestricted use, distribution, and reproduction in any medium, but not for commercial gain, provided the original author and source are credited.
