





Abstract
Over recent years hip arthroscopic surgery has evolved into one of the most rapidly expanding fields in orthopaedic surgery. Complications are largely transient and incidences between 0.5% and 6.4% have been reported. However, major complications can and do occur. This article analyses the reported complications and makes recommendations based on the literature review and personal experience on how to minimise them.
Introduction
Since the recognition of femoroacetabular impingement (FAI) as a common cause of hip pain,1 arthroscopy has evolved from an operation infrequently performed in the embryonic stages of development2 to an indispensable tool for treatment of FAI and many other intra- and extra-articular disorders.3
The hip is often considered the most difficult joint to arthroscope for several reasons4 including the need for special equipment, the local soft-tissue anatomy, and the contour of the articulating surfaces of the femoral head and the acetabulum necessitating mechanical traction in order to obtain access to the joint.2,5-7 Experienced hip arthroscopists have reported low rates of complications in large series, not exceeding 6.4%,6 and the majority of complications are transient.5,6,8 However, major complications can and do occur, requiring vigilance from the surgeon.
This is an overview of all potential complications associated with arthro- and endoscopic procedures in and around the hip joint. Based on the current literature and the authors’ experience, recommendations are provided on how these complications are best avoided.
Literature search
A literature search identified English-language studies using PubMed, Google Scholar and Science Direct. The keywords used were “complications in hip arthroscopy”, “revision hip arthroscopy” and “…hip arthroscopy”, where the term describing a complication was added at the beginning of the key term “review articles in hip arthroscopy”. All study types were included, including case reports and review articles, with no time limits applied. Eligibility was judged by consensus between the two authors, based on the title and abstract. Additional studies referenced in the selected papers were retrieved individually. Textbooks available to the authors were also explored. Study quality was not assessed.
Traction-related injuries
During arthroscopy of the hip, mechanical traction is necessary to separate the femoral head from the acetabulum and thereby provide space for the introduction of the arthroscope and instruments. This can lead to soft-tissue injuries associated with the traction itself (distraction-type) or with the perineal post used to provide countertraction (compression-type). These injuries are the most commonly reported complications of hip arthroscopy.9
Distraction-type
Distraction-type injuries are the most commonly reported complication of hip arthroscopy,9-11 reaching rates of up to 7% in small series.12,13 They are usually associated with prolonged procedures and/or use of excessive traction force, and almost invariably present as transient nerve palsies in the form of neurapraxia. More recent improvements in surgical techniques and development of specialised hip distractors have led to lower incidences compared with the early days of hip arthroscopy.
Patient positioning and duration of traction are the primary considerations. For arthroscopy of the central compartment, the extremity should be placed in slight hip flexion. This relaxes the anterior capsule2 and avoids full extension or excess flexion, which, when combined with traction, may endanger the femoral and sciatic nerves, respectively.5,14 Generally, traction of lower extremities in orthopaedics is likened to a tourniquet4,15: it should not exceed two hours of continuous application,6,15 with intermittent traction strongly recommended if a longer operating time is required.6,12
Once access has been obtained in a well-distended joint, traction may be reduced intra-operatively with little loss of distraction of the articulating surfaces. Griffin and Villar5 have attributed this to the creep properties of the capsular structures. They proposed a ‘trial of traction’ to minimise the duration. This involves applying traction temporarily to ensure the hip is distractible, then releasing traction during preparing and draping the operative field, and re-applying it when the operation starts.5 They described a rate of traction-related complications of 0.8% (four transient palsies of the sciatic nerve) in 640 consecutive hip arthroscopies.5 Others have adopted this recommendation,9 including the authors of the current review.
Traction neurapraxia is considered a benign complication, usually resolving fully and quickly within hours from surgery.5-8 The sciatic and femoral nerves are most vulnerable to undue traction, but no cases of permanent sequelae have been reported. Sampson6 described ten cases involving the peroneal nerve, all occurring early in the learning curve of two surgeons, which were attributed to the use of suboptimal distractors. To our knowledge, no other cases of peroneal nerve involvement have been reported. The lateral femoral cutaneous nerve is also susceptible to these injuries, but is generally considered more vulnerable to direct injury from the skin knife or instruments introduced through the anterior portal.
The “invasive hip distraction technique” has been proposed in order to minimise the occurrence of traction-related complications.16 This employs a spanning external fixation device to apply traction focused on the hip joint only, thereby avoiding the need for a perineal post and extending the acceptable traction duration: up to 270 minutes of traction has been reported in over 2000 cases with no traction-related nerve lesions.10 Spontaneously resolving haematomas at the level of the distal Schanz screws have occurred rarely.16
Recommendations
Continuous traction should not exceed two hours, with intermittent traction used in prolonged procedures.
The force should be limited in most cases to < 22.7 kg (50 lbs).
‘Trial of traction’ can reduce the total traction time.
Compression-type
These injuries are associated with the compressive force, usually exerted by the perineal post, used to provide countertraction. They are localised in the area of the groin where the pudendal nerve is primarily at risk, although one case of crural nerve palsy has also been reported.17 Pudendal nerve injuries have been reported since the first descriptions of modern hip arthroscopy.18 Other soft tissues may be affected, including the scrotum and the labia majora, with injury ranging from oedema19 or haematoma formation7 to pressure necrosis.17,19,20
Glick et al18 attributed this complication to the compression of the rami against the perineal post in hip arthroscopy, although this injury and mechanism is not unique to hip arthroscopy. The orthopaedic trauma literature abounds with reports of catastrophic injuries, including crush syndrome of the thigh,21 attributed to a malpositioned perineal post or prolonged traction.15,21,22 Reversible erectile dysfunction has been described in trauma patients with post-operative pudendal nerve lesions,15 but not in arthroscopy. Brumback et al23 prospectively studied the pressure in the perineal area in patients undergoing intramedullary nailing for femoral fractures using a traction table. Traction duration did not correlate with pudendal nerve injury (2.6 hours vs 2.8 hours, p = 0.15) but a significantly higher traction force was found in affected patients (73.3 kg-hours vs 34.9 kg-hours, p < 0.03): they concluded that magnitude rather than duration of traction predisposed to injury of the pudendal nerve.23
Brumback et al23 also reported that adduction at the hip increased the traction force.23 This may explain the relatively lower incidence of pudendal nerve injuries in hip arthroscopy, as hip abduction is typically employed to relax the capsule and facilitate entry. Hip adduction increases forces around the perineal post24; in awake volunteers in the supine position, these forces were reduced by 50% with hip abduction.25
Recognition of these injuries has led to the development of hip arthroscopy techniques without a perineal post. No complications occurred in a group of 30 patients undergoing hip arthroscopy using a deflated beanbag and taping instead of a perineal post.26 In the same report, the authors questioned the long-held belief2,27 that a lateralised force must be applied through the perineal post in order to obtain an overall traction force vector in line with the femoral neck.26
Nevertheless, use of the perineal post remains standard practice in hip arthroscopy performed in the lateral or supine position. To prevent compression-type compression injuries, a well-padded post, wide enough (diameter ≥ 9 cm) to distribute the forces over a larger area of the skin, should be positioned against the medial thigh (not the groin crease and genitalia).3,6,9,27 Distraction devices are now available using perineal posts of up to 9 inches in diameter.28 The lateral force exerted by the post should not be excessive; in women there is a risk of vaginal tears.5 The magnitude of the traction force should ideally be kept to a minimum: muscle relaxants should be used9,10 and arthrocentesis performed as soon as possible2,7 to neutralise the resting negative intra-articular pressure.2,20 Fluid distension further distracts the articulating surfaces without increasing the traction force.29 Patients with conditions that limit distraction of the hip joint are at increased risk of these complications and should undergo hip arthroscopy only by experienced surgeons. Although reported forces required for traction have varied,2,7,20 a maximum of 22.7 kg (50 lbs) should suffice for most patients.2-4,9,29
Undue pressure on the ipsilateral foot, ankle and leg, usually when a boot is used, may also be considered a form of compression-type injury. The foot is prone to inadvertent compression when placed tightly in a boot, particularly in thin patients (Fig. 1). Diminished sensation in the distribution of the superficial peroneal nerve has been reported,30 as well as vascular obstruction of all three major arteries at the ankle level.31 The foot should be well-padded, especially around the bony prominences of the malleoli.6,31 Some surgeons prefer the use of a foot plate.26

Fig. 1
Photograph of a right leg after a two-hour uncomplicated hip arthroscopy using a boot and a dedicated hip distractor. Despite adequate padding, there are signs of excess pressure on the skin overlying the lateral malleolus and the mid-calf. All pressure marks had resolved upon discharge a few hours later.
Recommendations
The perineal post and foot plate/boot must be heavily padded.
The perineal post should be ≥ 9 cm in diameter, positioned against the medial thigh rather than the groin crease.
The extremity should be positioned in slight abduction.
The scrotum and labia majora should be inspected both before and after application of traction to ensure they are not entrapped or everted.
The lateral force vector exerted by the post should not be excessive, especially in women.
Iatrogenic chondral and labral damage
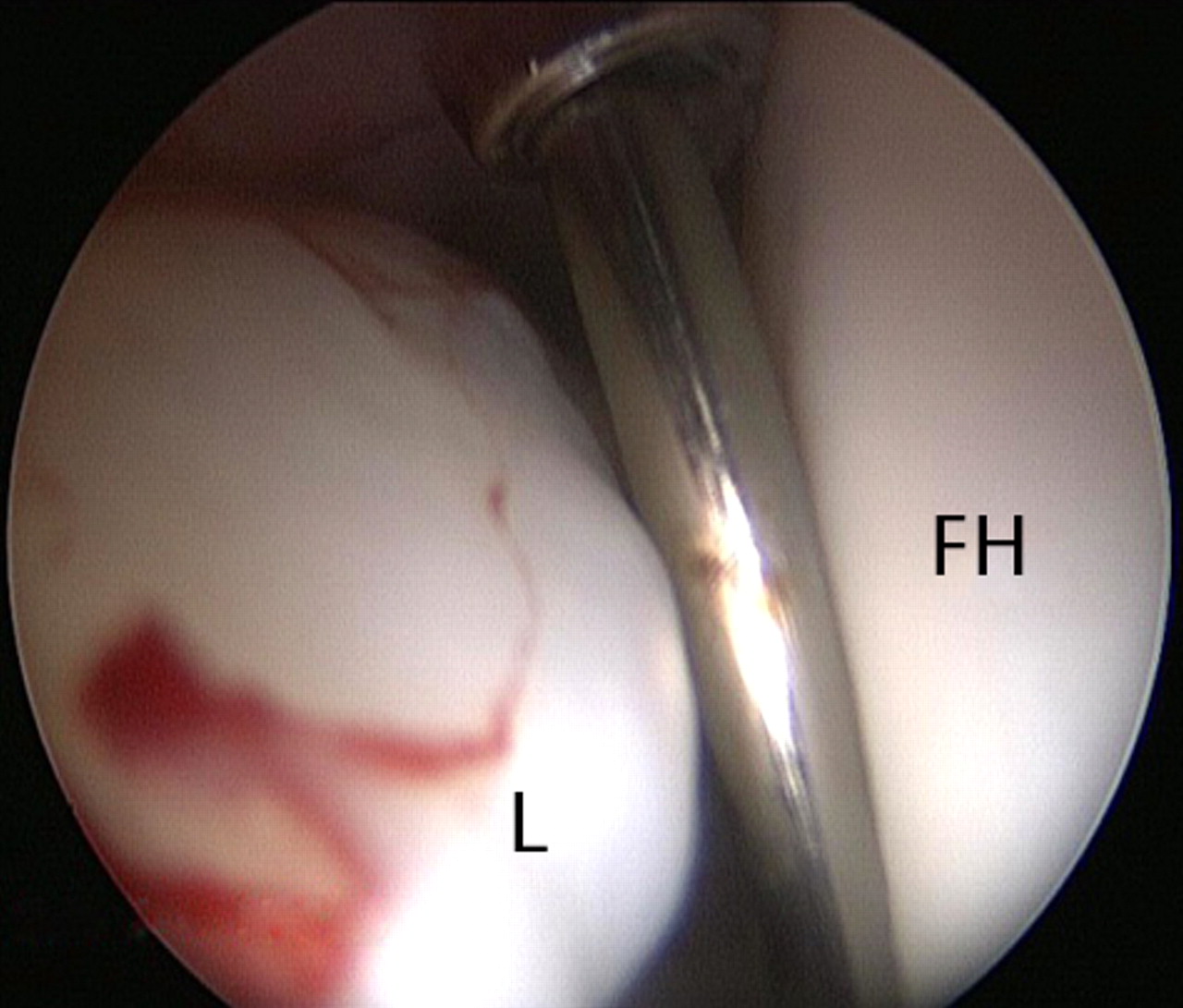
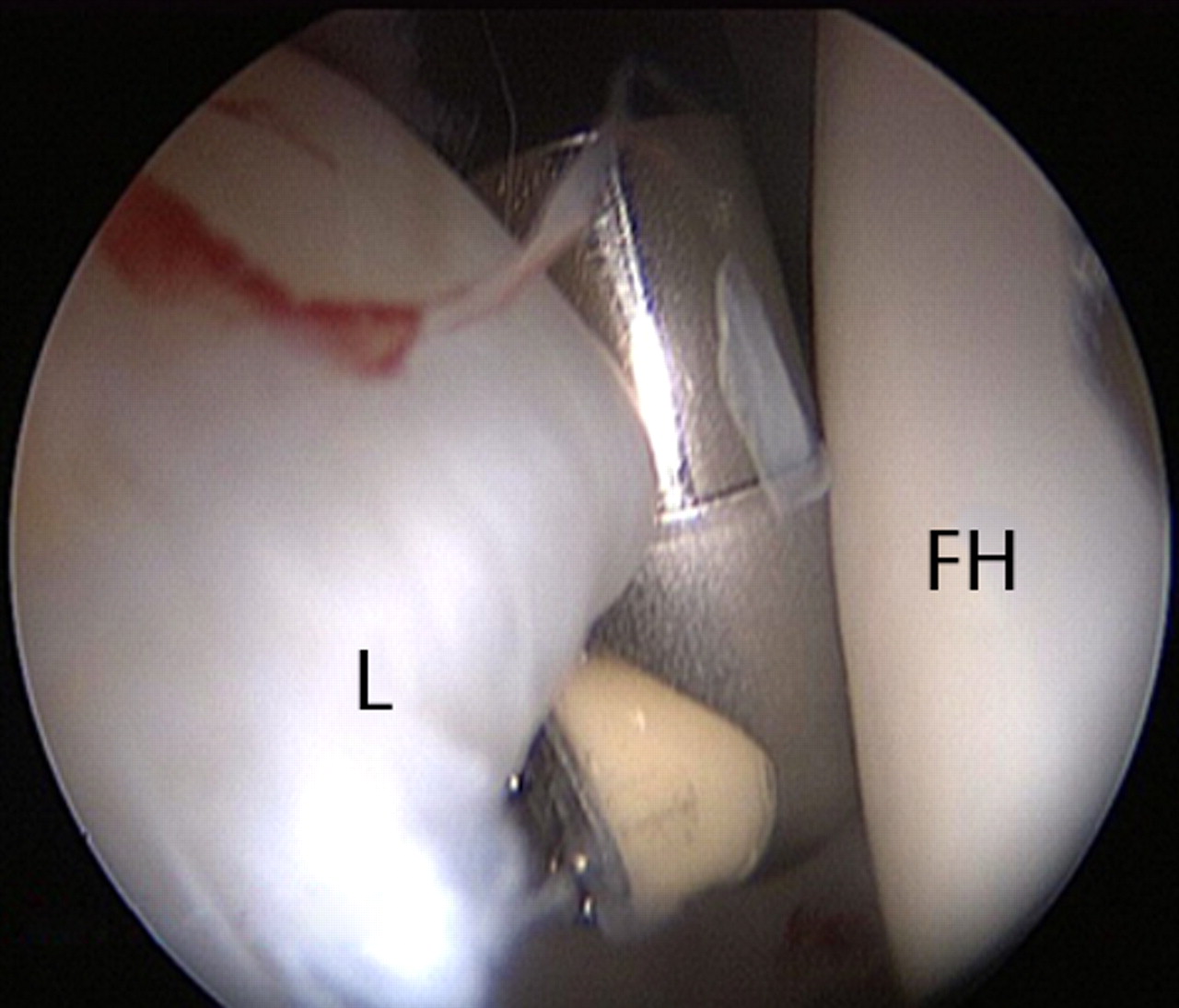
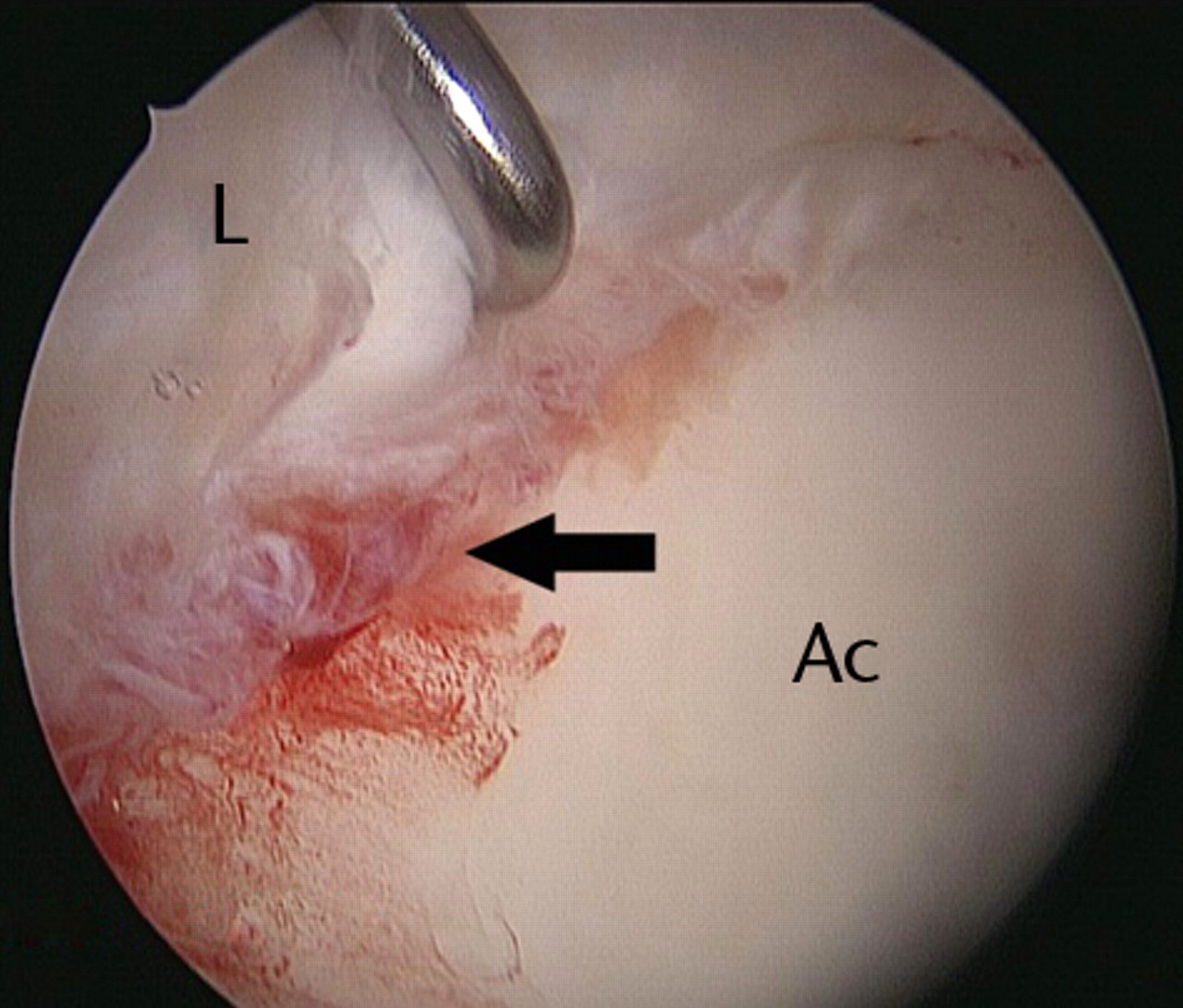
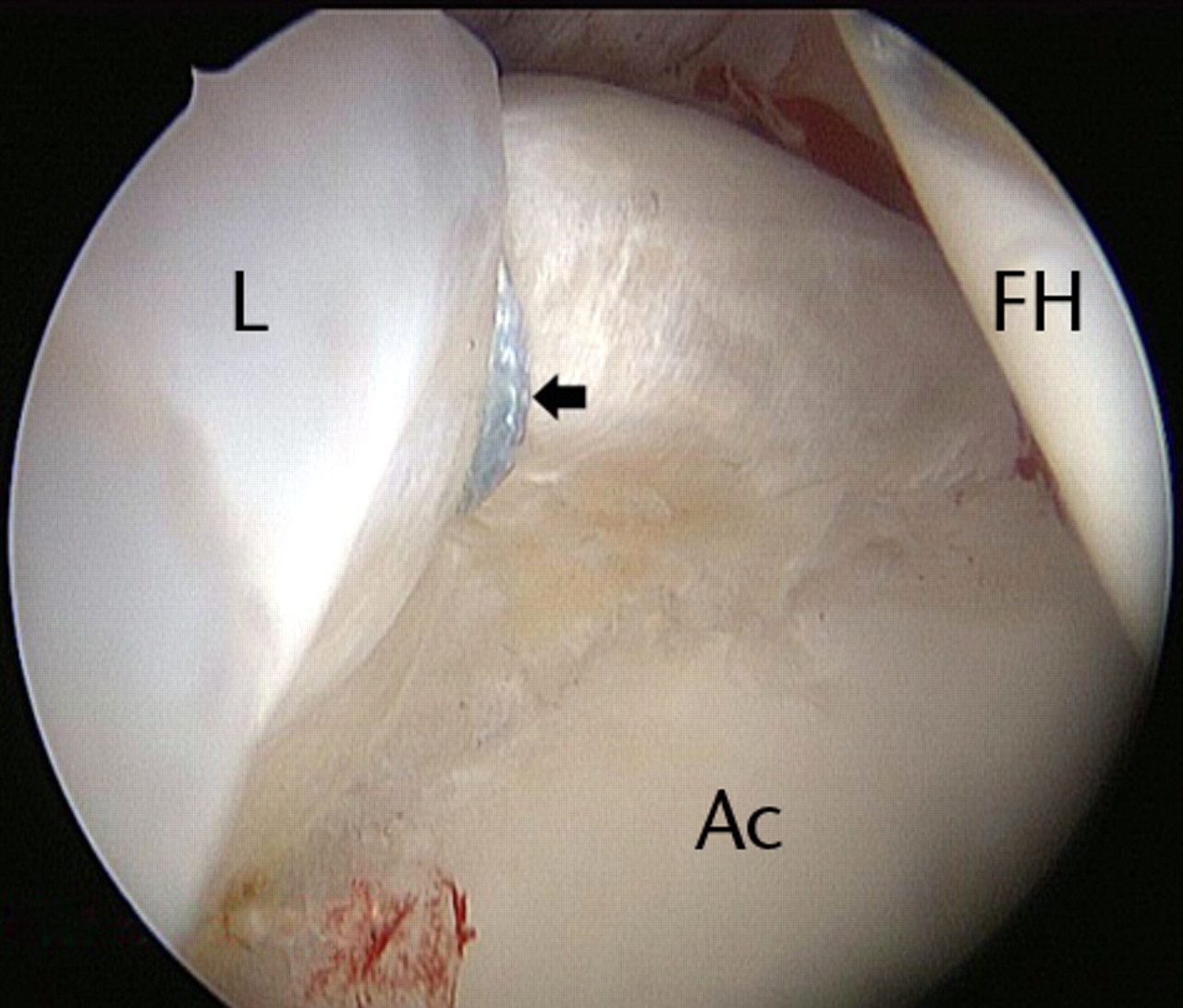
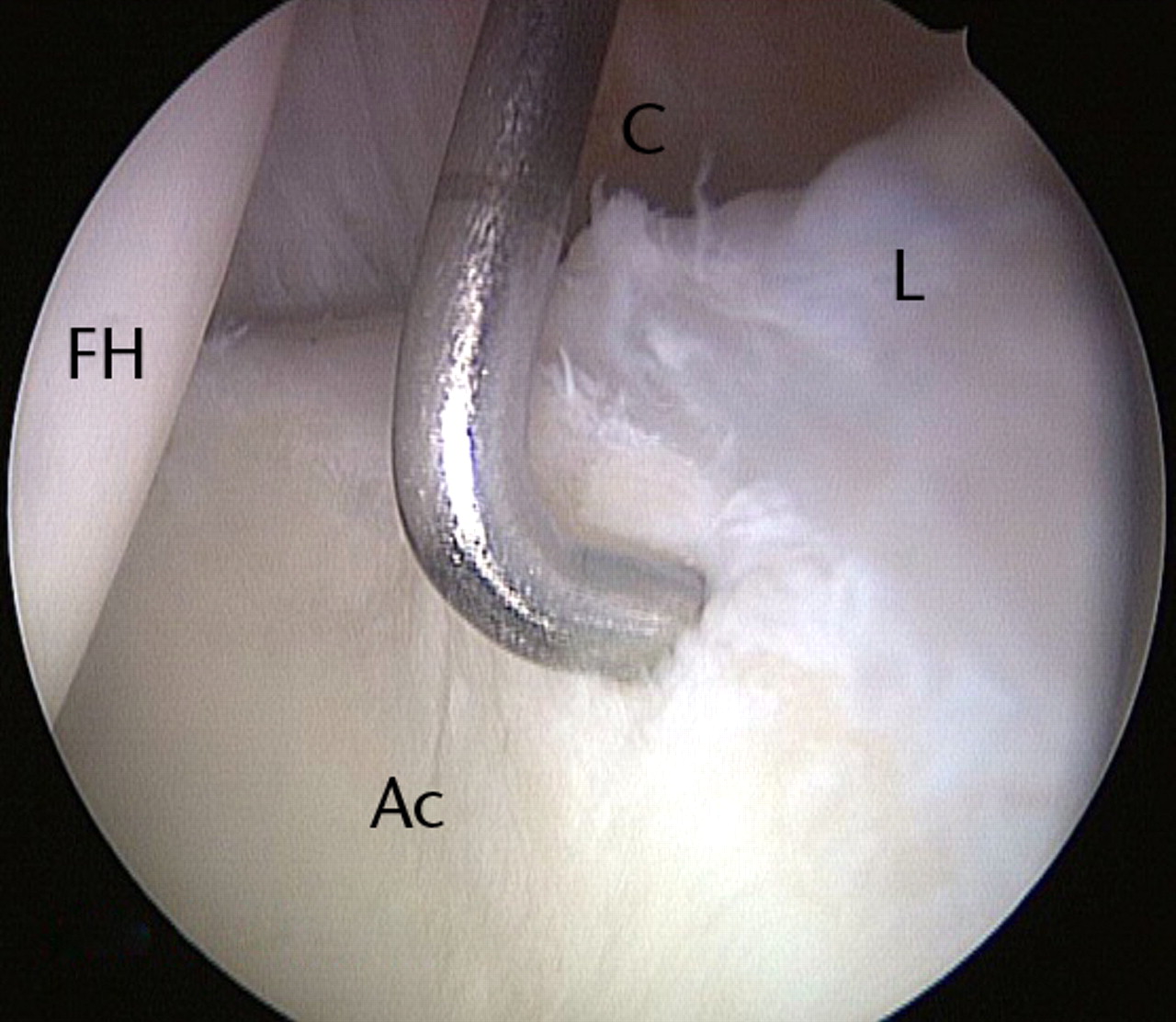
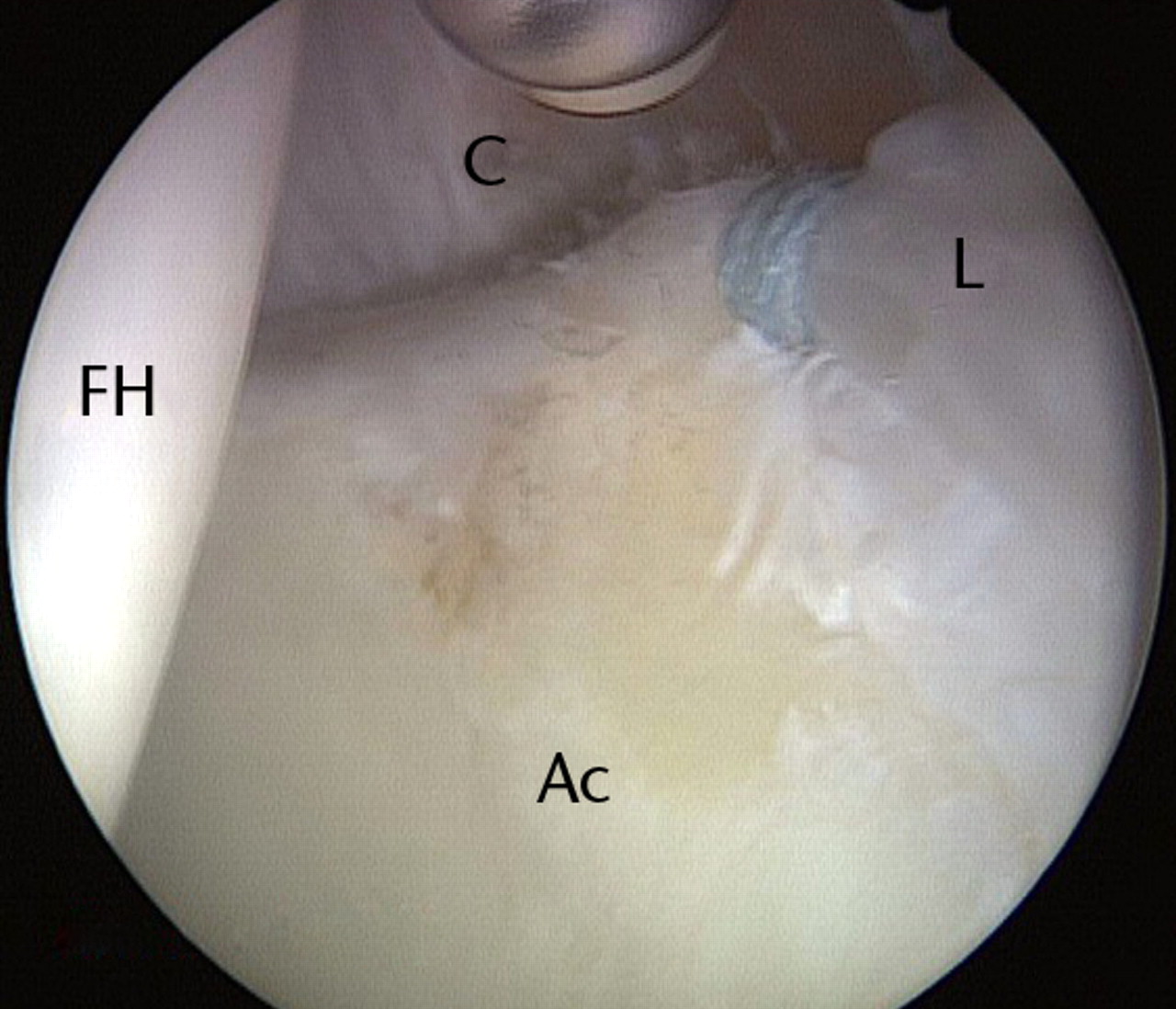
Iatrogenic injury to the cartilage and labrum is relatively common in hip arthroscopy, but underreported.32 Typically, the superior or anterosuperior labrum is inadvertently punctured in establishing the anterolateral portal. Although this is performed using a modified Seldinger technique,10 this ‘blind stick’ is not fool-proof.33 The labrum corresponding to the anterior portal may also be injured when visualisation is poor (e.g., in the presence of severe synovitis). Caution is recommended when accessing dysplastic hips: although easily distractible, the hypertrophic labrum makes instrumentation difficult. Labral detachment, in which the labrum occupies more of the joint space, exacerbates this problem (Fig. 2).
Figs. 2a - 2d
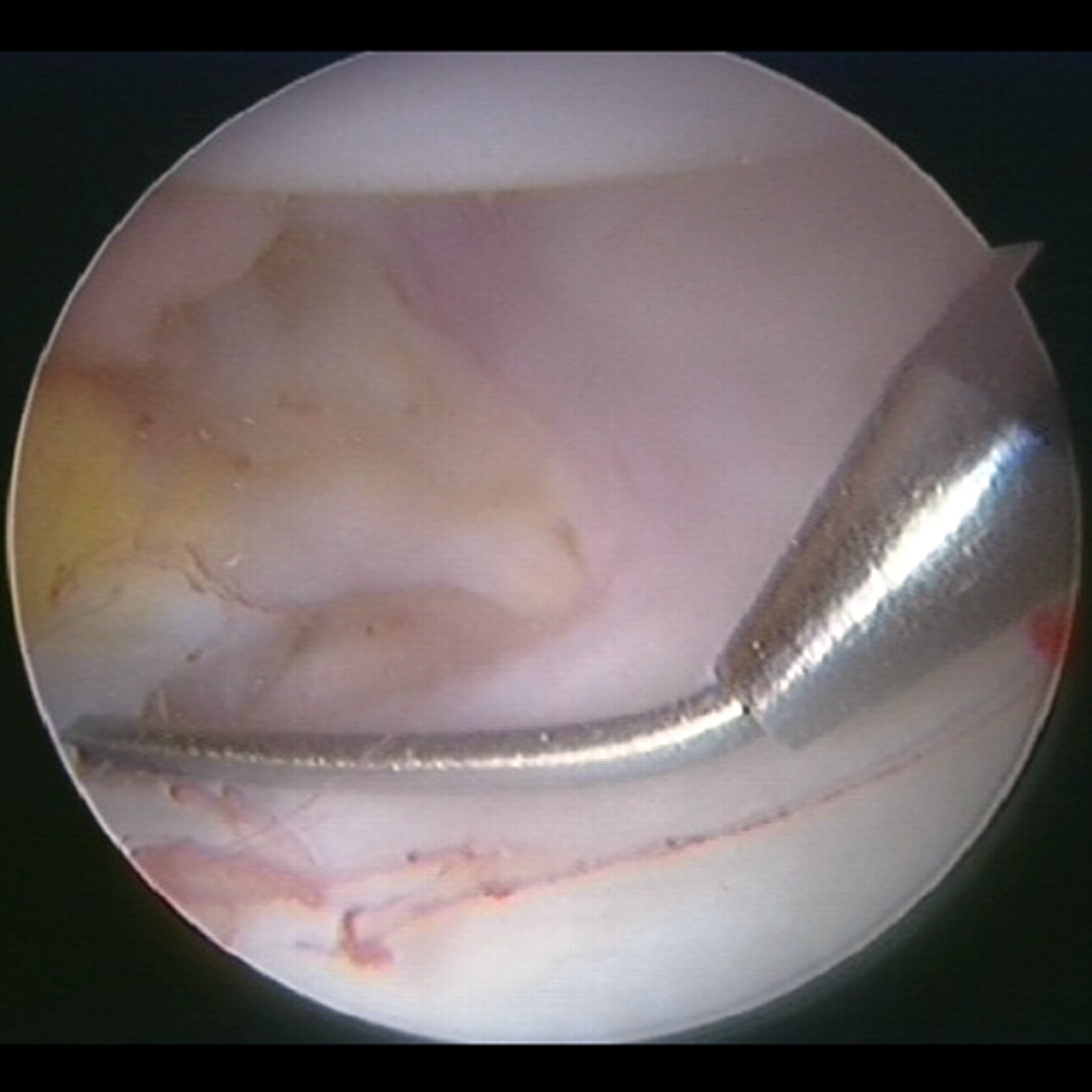
Arthroscopic images of the right hip of a 53-year-old woman with mild dysplasia, showing a) significant hypertrophy of the anterosuperior labrum, leaving little room for the 5 mm dilator and guide wire inserted through the anterior portal, b) the radiofrequency ablation probe just interposed safely between the labrum and the femoral head, c) partial labral detachment (arrow), and d) improved visualisation after labral repair with a suture anchor (arrow) (L, labrum; FH, femoral head; Ac, acetabulum).
Chondral scuffing usually affects the femoral head.34 Inadequate traction has traditionally been cited as the main cause of these injuries.6,8,35 However, iatrogenic injury to the femoral head may also occur in complex cases involving repetitive exchange of instruments, despite adequate distraction (Fig. 3).
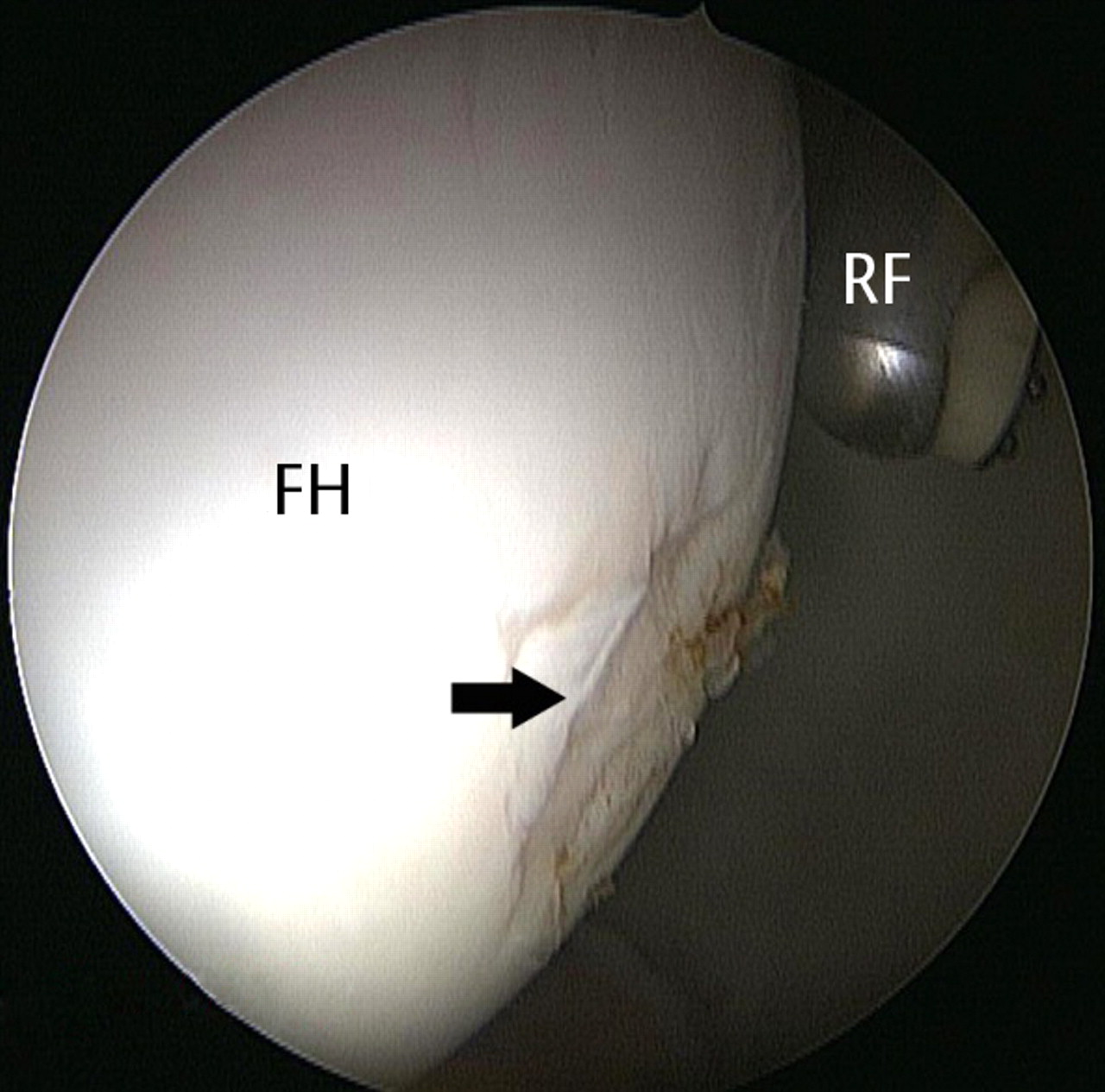
Fig. 3
Arthroscopic image showing iatrogenic partial-thickness chondral scuffing (black arrow) of the femoral head (FH) in a 40-year-old man undergoing labral repair with three suture anchors. The radiofrequency ablation probe (RF) was used to smooth the scuffed area of the femoral head.
Clarke et al8 considered access difficult in 18% of 1000 hip arthroscopies, and iatrogenic labral or chondral injuries could have occurred in these. Sampson6 reported three cases with significant scuffing of the femoral head due to inadequate distraction in 1000 arthroscopies, but considered that needle and instrument manoeuvring would result in minor scuffing without permanent damage in most hip arthroscopies. McCarthy and Lee35 identified a 3% rate of mild chondral scuffing, which was associated with difficult distraction (e.g. protrusio deformity, degenerative joint disease). Higher rates of chondral scuffing have been reported by lower-volume arthroscopists.12 Ilizaliturri et al36 described 100 patients at two years, 68 of whom sustained small cartilage lesions during hip arthroscopy. They concluded that partial-thickness, instrument-produced cartilage injury was very common, with no appreciable impact on short-term results.36
Badylak et al,37 in 250 consecutive hip arthroscopies, identified 50 patients (20%) with iatrogenic labral punctures, which did not affect the one- or two-year clinical results. The literature accepts that occasional iatrogenic damage to the cartilage and labrum is inevitable, but attention to detail and surgical experience should minimise this risk.33
Recommendations
Distraction ≥ 10 mm followed by intra-articular injection of 20 ml to 40 ml of normal saline for fluid distension are advised for safe access. The ‘Byrd sign’ (distal movement of spinal needle with injection of saline) can be false-positive in 42% of cases.37
The spinal needle should always be inserted with its bevel towards the femoral head; both tactile and visual feedback are important in avoiding the labrum.10
It is recommended to briefly exchange portals with the camera, in order to verify that the labrum has not been punctured by the cannula.
If adequate distraction cannot be achieved (common in arthritic hips), the peripheral compartment should be accessed first, to allow for placement of the guide wire into the central compartment under direct vision.38
Fluid extravasation
Leakage of the irrigation fluid into anatomical spaces adjacent to the joint is a dangerous complication of hip arthroscopy. In intra-capsular hip arthroscopy, the fluid escapes through capsular incisions,39,40 although most reported cases involve extra-capsular endoscopic procedures (typically release of the psoas tendon)41-43 or the presence of a fresh acetabular fracture44; however, another group did not report similar problems in a series of 11 fractured hips.45 Often, but not always, the operating time in these cases has been prolonged.39,43 No extra-capsular cases involving the trochanteric compartment have been implicated in abdominal fluid extravasation. The exposed iliopsoas sheath may act as a conduit for fluid to leak into the retroperitoneum and ultimately the peritoneal cavity.42
Three cases of femoral nerve palsy with long-term sequelae have been described secondary to extravasation into the thigh during knee arthroscopy46 but no similar cases have been reported in hip arthroscopy. Of more relevance to hip arthroscopy is the escape of fluid into the abdomen. Fluid volumes between 2 and 3 litres in the retroperitoneum and abdomen have been reported in symptomatic patients.39 The tell-tale clinical sign is abdominal distension, sometimes with subcutaneous oedema of the thigh and hypothermia.39,42 If surgery is performed under regional anaesthesia, abdominal pain may develop intra-operatively and lead to early termination of surgery.7 Otherwise, abdominal pain develops in the acute post-operative period.40 Seizures of unknown aetiology were reported by Haupt et al.39
In cases performed under general anaesthesia, continued accumulation of abdominal fluid may lead to compartment syndrome, necessitating emergent laparotomy.41,43 In any case of extravasation into the abdomen, an urgent general surgical consultation should be sought. Diagnosis is confirmed with ultrasound39 or CT.40,42 One case of fluid extravasation into the thorax has been reported42; post-operative shortness of breath may not only signify pulmonary embolism.
Fluid extravasation has been linked to the arthroscopic equipment used; normal saline used as irrigation fluid has been blamed, but this issue is contentious.47 Sampson6 described ten mild cases of extravasation in early arthroscopic experience and recommended the use of an outflow-dependent pump. A pressure-sensitive system has also been recommended.7,29,48
However, excluding a 1998 case report,44 most severe cases of fluid extravasation are recent, with modern equipment,40,42,43 possibly due to the increasing volume and complexity of hip arthroscopies. Early literature on hip arthroscopy suggested that some fluid inevitably escapes into the abdomen to be subsequently resorbed.7 Stafford, Malviya and Villar49 recently reported a mean extravasation of 1132 ml (95% confidence interval (CI) 808 to 1456) of irrigation fluid into peri-articular tissues. The surgeon should always be aware of the ingress–egress balance of irrigation fluid during the procedure.14 Abdominal examinations pre- and intra-operatively have been recommended.48 Given its potential implications, fluid extravasation should be discussed with all patients undergoing hip arthroscopy and should feature on consent forms.40
Recommendations
Surgical time should be kept to a minimum and capsulotomies used sparingly.
Inflow fluid pressure should be low (40 to 50 mmHg) and fluid balance monitored.
The procedure should be abandoned if there are signs of extravasation threatening the patient’s general condition.
It is safer to defer hip arthroscopy until a recent acetabular fracture has united.
Endoscopic release of the psoas, if planned, should be performed last.
Intra-operatively, the abdomen and core body temperature should be closely monitored.
Infection
There is one report of septic arthritis following hip arthroscopy.8 In 218 hip arthroscopies performed in children and adolescents, Nwachukwu et al50 reported one case of suture abscess in a proximal portal of a patient undergoing arthroscopy for Perthes’ disease.
Hip arthroscopy lasts for approximately two hours and can involve fairly extensive soft-tissue dissection, bony reshaping and the use of foreign materials (e.g., implants for labral fixation, sutures for capsular plication). Moreover, it is occasionally performed in the presence of hip replacement components. Chemoprophylaxis in hip arthroscopy has not been specifically studied, and to our knowledge there are no current recommendations. However, routine administration of broad-spectrum antibiotics pre-operatively is advised to prevent this exceedingly rare but serious complication.48
Recommendations
Administration of a single dose of intravenous broad-spectrum antibiotic at induction.
Deep-vein thrombosis
Hawkins51 in 1989 warned of the possibility of thromboembolic episodes and even pulmonary emboli complicating hip arthroscopy. A review of several large series found a 0% rate of deep-vein thrombosis (DVT) or pulmonary embolism (PE) in over 5500 patients.52 However, individual thromboembolic events have been reported, either in relation to known predisposing factors, such as Factor V Leiden deficiency35 and use of oral contraceptives (where DVT occurred on the non-operated extremity and involved the left common femoral, superficial femoral and popliteal veins),28 or in the absence of known risk factors.19 In a retrospective review of 81 patients (81 hips) undergoing arthroscopy, three patients (3.7%) developed symptomatic DVT post-operatively confirmed by Doppler ultrasound53; all resolved with treatment, leaving no residual long-term problems. A retrospective study of 35 patients (35 hips) revealed one case of DVT. However, femoral osteochondroplasty in those patients was performed through a limited open approach.54
The only known case of fatal PE after hip arthroscopy was in a polytraumatised 32-year-old male with a shooting injury to his lower abdomen, a resultant small retroperitoneal haematoma and fracture of the ilium.52 He underwent exploratory laparotomy and percutaneous fracture fixation prior to arthroscopic removal of loose bodies from the hip. Thus, we believe the link between the PE immediately post-operatively and hip arthroscopy is far from clear in this case.
Both authors have each had one patient with confirmed DVT approximately one week following hip arthroscopy, and are aware of other cases experienced by colleagues. We believe that the true incidence of thromboembolism after hip arthroscopy is either underreported or unrecognised, with no formal guidelines on the need, type or duration of thromboprophylaxis. More research is certainly needed.
Recommendations
Early post-operative mobilisation (ideally on the day of surgery).
Use of below-knee elastic antithrombotic stockings on the contralateral extremity intra-operatively.
Pharmacological prophylaxis administered on an individualised basis, depending on predisposing factors (age, family or personal history of DVT or PE, obesity, smoking, blood disorders).
Possible discontinuation of oral contraceptive use prior to hip arthroscopy.
Instrument breakage
The thick soft-tissue envelope around the hip makes manipulation of the arthroscope and instruments difficult, even in the presence of distraction.5 The curvature of the articular surfaces poses further problems and also predisposes to instrument bending or breakage,6 demanding careful and gentle handling. Traditionally, the guide wires used for insertion of cannulae have been thought to be most at risk, although other instruments may sustain mechanical failure55 including the tip of the arthroscope.5 The guide wires are made of nitinol, a shape memory nickel-titanium alloy that allows for substantial elastic deformation before failure.56 Obviously, breakage is still possible and usually occurs when a cannula is forcibly inserted over a bent guide wire, shearing off the guide wire (Figs 4a and 4b).57 Extreme caution is required when inserting guide wires into the peripheral compartment; this is probably the hardest and most dangerous area to retrieve broken guide wires from, especially when they have migrated through the medial capsule (Fig. 4c).10


Figs. 4a - 4c
Image intensifier (a) and arthroscopic (b) images showing the insertion of a cannulated 4.5 mm trocar over a bottomed out nitinol guide wire, and c) a bent nitinol guide wire inserted into the peripheral compartment and past the medial capsule of the hip. A broken guide wire in that area is difficult to retrieve.
Broken instruments may also be difficult or impossible to retrieve from the central compartment (Fig. 5). Griffin and Villar5 described an irretrievable broken jaw of a forceps that had to be pushed into the cotyloid fossa and abandoned, with no adverse sequelae for the patient. The presence of osseocartilaginous fragments in the same region with no detriment for the patient has been described by Bartlett et al.44 Moving loose bodies or broken instruments away from the weight-bearing area of the hip joint and into the cotyloid fossa seems to be an effective strategy, should these prove to be irretrievable.
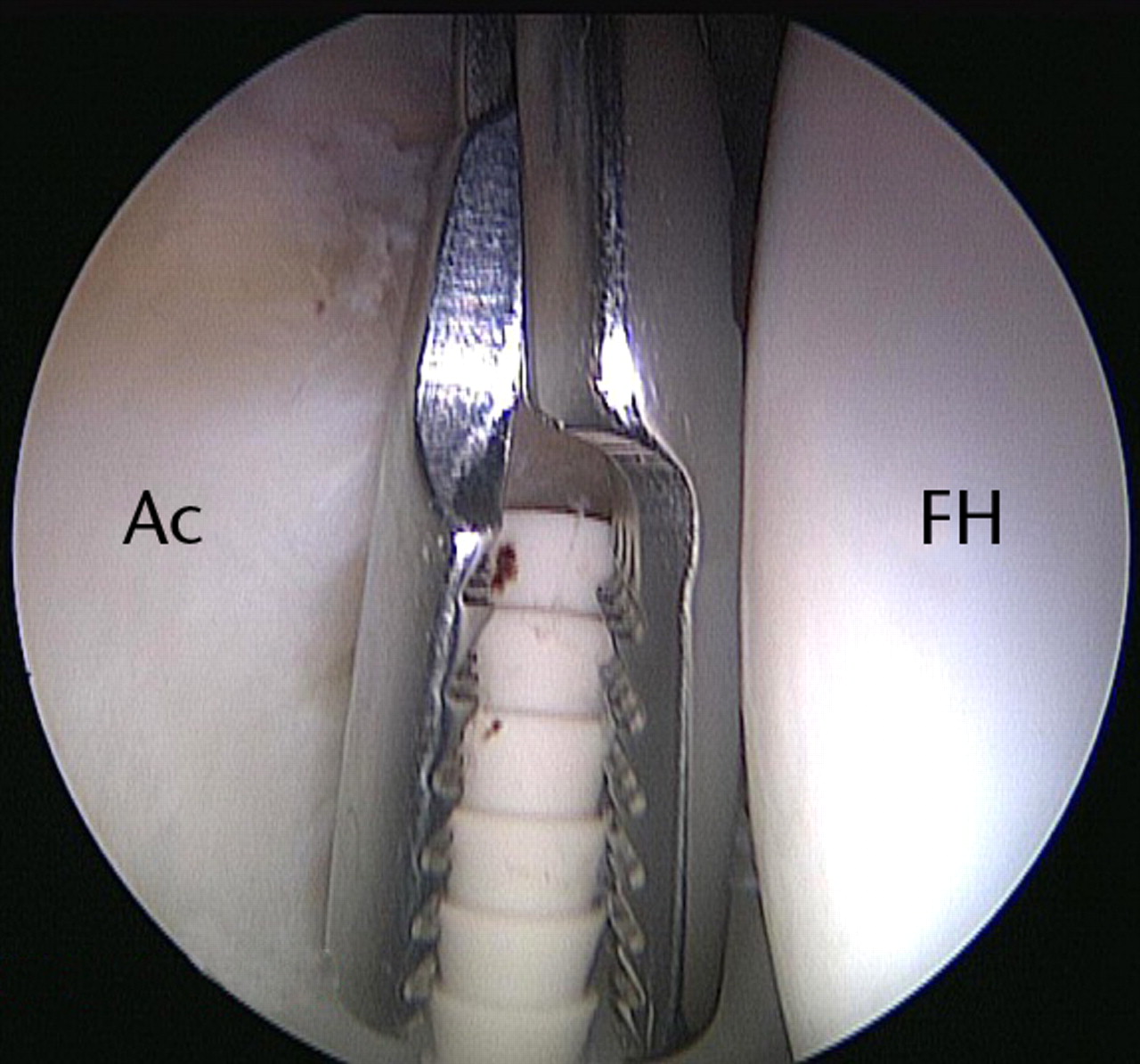
Fig. 5
Arthroscopic image showing retrieval of a broken suture anchor from the anterior joint space of the central compartment during attempted labral repair (FH, femoral head; Ac, acetabulum).
Recommendations
A bent guide wire must be retracted gently during careful and controlled insertion of the cannula.
Instruments must be manipulated carefully, especially in a tight joint.
Avascular necrosis of the femoral head
Avascular necrosis (AVN) following hip arthroscopy is more a theoretical concern than a true clinical problem.32 The same holds true for the progression of already established AVN,58 which has been described once after hip arthroscopy.2 Sampson6 reported the case of a 36-year-old male who developed AVN seven months following partial labrectomy and debridement after an injury at work. Although the hip might have been already at risk due to the original injury, the distraction and partial capsulectomy may have further contributed to the event.6 A case report described a 24-year-old patient without any risk factors for AVN who underwent debridement of the labrum and decompression of a pincer lesion.59 The operation was uneventful and within usual time limits (traction duration 90 minutes), not requiring any excessive distraction force or fluid pressure. AVN was attributed to the vascular compromise caused by traction.59 Traction was also implicated in the causation of AVN in a 61-year-old woman, three months after partial arthroscopic labrectomy.60
Factors linked to AVN after hip arthroscopy include distraction, partial capsulectomy and insult to the lateral epiphyseal branch of the medial femoral circumflex artery,6 which is critical for the vascularity of the femoral head.61 AVN has also been reported in young children undergoing arthroscopic reduction for developmental dysplasia of the hip (DDH).62,63 It has been postulated that release of the iliopsoas might prevent this complication.63 In this unique patient population, hip arthroscopy is performed without traction.62,63 It is probable that the mere reduction of the head into the acetabulum compromises the blood supply to the femoral head, rather than the arthroscopic procedure, as the same complication is known to occur after open reduction.
Femoral osteochondroplasty for cam deformity is considered to most imperil the vascularity of the femoral head, by extending too far laterally.6,32 In the peripheral compartment, the lateral synovial fold is a reliable landmark used in hip arthroscopy for identifying the branches of medial circumflex artery that lie behind it; the lateral extent of femoral osteochondroplasty should terminate just before this fold.32
Recommendations
Capsular dissection or bony resection posterior to the lateral synovial fold in the peripheral compartment is to be avoided.
Portal-related complications
The hip joint is surrounded by several neurovascular structures, including the femoral neurovascular bundle anteriorly, the lateral femoral cutaneous nerve (LFCN) anterolaterally and the sciatic nerve and gluteal vessels posteriorly.2 With the exception of the LFCN, direct neurovascular injury is very rare, although great care is needed to avoid a potentially devastating injury to any of these structures.14
The proximity of neurovascular structures to portals and the effect of traction on their spatial relationship have been investigated. Findings that traction may fix and lateralise neurovascular structures, rendering them more susceptible to direct iatrogenic injury,64-66 have not been confirmed by recent investigations. A cadaver study of 16 hips found 22.7 kg (50 lbs) of traction to have little deleterious effect on the anatomic location of neurovascular structures, but the femoral and sciatic nerves were noted to move away from the anterior and posterolateral portals, respectively.67 In the same study, the LFCN was found to move closer to the anterior portal by a mean of 0.22 mm after application of traction (5.0 mm vs 4.78 mm, p > 0.05). The overall safety of arthroscopic portals for hip arthroscopy was also confirmed in an investigation in ten cadaveric hips.68
The structure most at risk for direct injury is the LFCN, which lies very close to the anterior portal in line with the anterior superior iliac spine.9 Robertson and Kelly68 described a modified anterior portal, 1 cm more lateral, at a safer distance from the LFCN (mean 15.4 mm (1 to 28)). However, they cautioned against stab incisions for the anterior portal due to the variable branching pattern of this nerve.68 Other surgeons place the anterior portal even more laterally to protect the LFCN.10 Standard practice should comprise a lateralised anterior portal and cutting no deeper than the deep dermis with the knife.
Vascular injuries
Minor bleeding is common during hip arthroscopy, but is easily controlled either with a transient increase in fluid-pump pressure or with coagulation at the source using the radiofrequency (RF) ablation probe. Griffin and Villar5 described a case of bleeding from an arthroscopic portal after injury to a superficial vein, which ceased after 48 hours of external pressure, and a patient with haematoma of a portal. Late bleeding at several weeks post-operatively has also been described, attributed to laceration of a branch of the superior gluteal artery.10 It resolved with conservative treatment.
We are aware of one reported serious vascular complication with long-term sequelae. Incorrect placement of the posterolateral portal severed the inferior gluteal artery in a 61-year-old woman, who presented with persistent anaemia and severe neurological dysfunction after hip arthroscopy for osteoarthritis.69 A large pseudoaneurysm compressing the sciatic nerve was found. Treatment with embolisation and decompression/neurolysis led to marked clinical improvement, but there was residual motor weakness affecting the anterior compartment of the leg after two years.69
Osteochondroplasty of the proximal femur for treatment of cam-type FAI involves the exposure of a relatively large surface area of raw, highly vascular cancellous bone of the head-neck junction, and minor intra-operative bleeding is commonly encountered. Although osseous in origin, it is useful to try to control this bleeding with the RF ablation probe after use of the high-speed burr (Fig. 6). This may reduce the post-operative haemarthrosis, speed up recovery, and even minimise adhesions between the capsule and the osteochondroplasty region, but supportive data are not available.

Figs. 6a - 6b
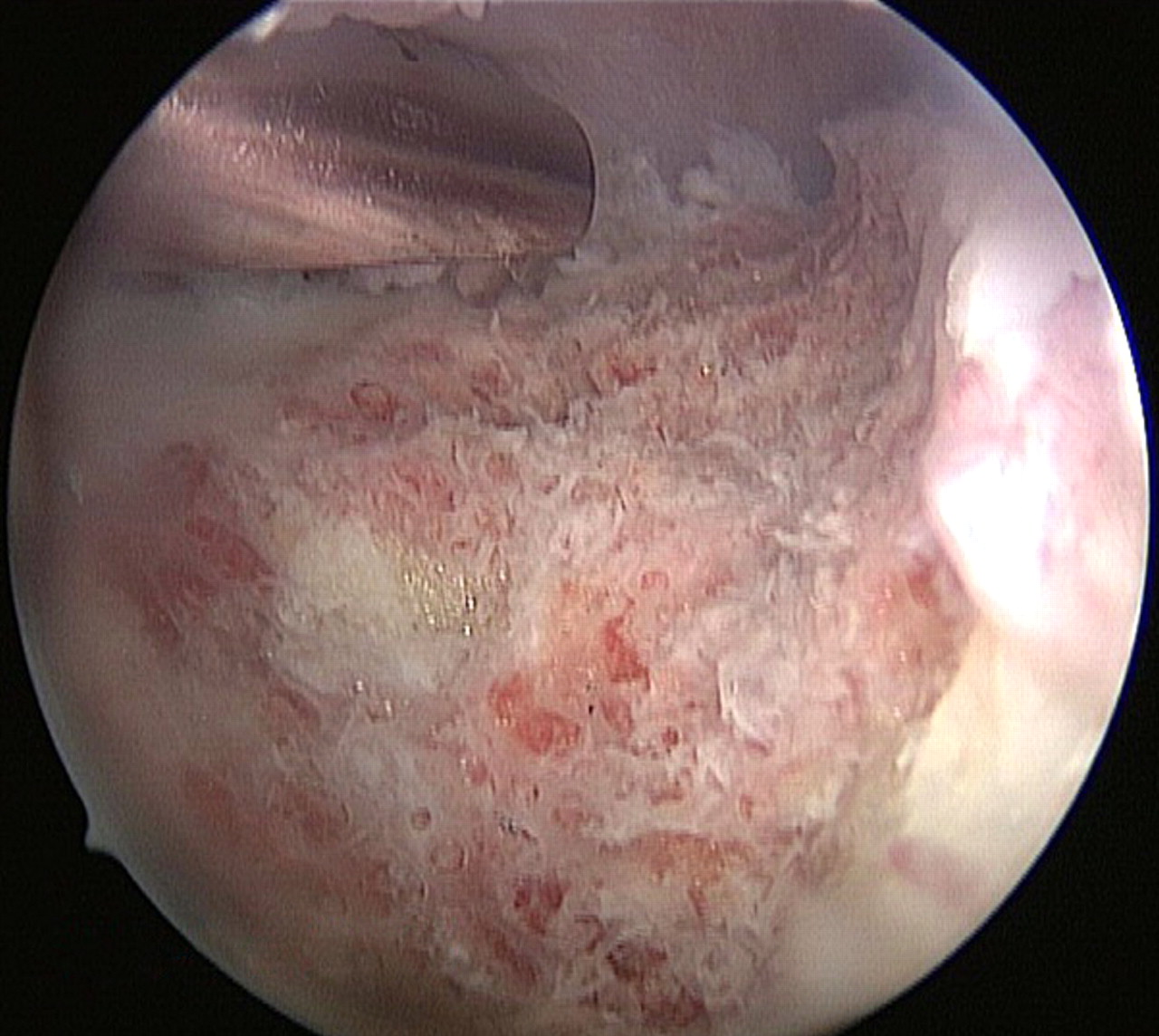
Arthroscopic images of the peripheral compartment of a left hip, a) after femoral osteochondroplasty, showing the exposed bleeding surface of raw cancellous bone, and b) after treatment with the radiofrequency ablation probe for haemostasis.
Nerve injuries
Direct nerve injuries attributed to suboptimal portal placement have only been reported for the LFCN. Any patient complaining of diminished sensation or numbness over the anterolateral thigh following hip arthroscopy should be considered to be suffering from LFCN injury until proven otherwise. Its incidence is difficult to define, as it is not always clear if reported cases are due to traction neurapraxia6 or direct laceration.34,70 In the absence of prolonged traction, we believe the latter is more likely. Byrd14 found the risk of injury to one or more branches of the LFCN, using the traditional anterior portal as described previously, to be 0.5%.
The implications of this complication have been described as minimal in patients undergoing hip replacement surgery through a direct anterior approach.71 This nerve usually does not recover70,71 and patients should be forewarned accordingly.
Rarely, major nerve injuries may develop secondarily, as a result of an adjacent vascular primary insult. The pathomechanism in this case involves direct local compression of the nerve by haematoma or a pseudoaneurysm.69
Recommendations
Neutral rotation of the limb during portal placement to ensure the anatomy is not distorted.
Bony landmarks such as the anterior superior iliac spine and borders of the greater trochanter should always be identified and marked.
A lateralised anterior portal is safer; the skin incision should not extend into the subcutaneous fat (“nick-and-spread” technique) because of the superficial course of the LFCN.
Internal rotation of the hip is to be avoided in placement of posterior portals.
Treatment of FAI: femoral neck fracture
Over-aggressive resection of the cam deformity has two potential adverse consequences: the loss of the sealing effect of the labrum in flexion72 and predisposition to iatrogenic femoral neck fracture. Mardones et al,73 in a cadaver study, suggested that 30% of the femoral neck diameter could be resected safely, although such resection decreased the energy required for a fracture. The resection undertaken in removal of cam deformity is usually to the depth of the normal neck profile, which rarely reaches 30% of the bone diameter32; femoral osteochondroplasty is generally safe.
There have been reports of three patients suffering femoral neck fractures after arthroscopic19,74 or arthroscopically-assisted75 correction of cam deformity. Two were middle-aged (5174 and 5675 years), sustained the fracture early post-operatively (three75 and five74 weeks) and both fractures were minimally displaced. Full weight-bearing75 or a sudden increase in physical activity74 occurred prior to the fracture. No similar data were provided for the third patient, although the authors proposed over-aggressive osteochondroplasty.19 Laude et al75 consequently modified their rehabilitation programme to include six weeks of protected weight-bearing, especially in patients with poor bone quality or aged > 40 years.
The amount of bone resected, the patient’s age and bone quality and the level of post-operative weight-bearing are thought to contribute to this complication. Osseous remodelling at the site of the femoral head-neck junction after osteochondroplasty has been described in 113 hips undergoing the limited open procedure with toe-touch weight-bearing for six weeks.76 Complete recorticalisation of the resected margins was observed in ten hips at a mean of 20 months (8 to 54), but only partial or no recorticalisation was seen in 88 and 15 hips, respectively. Importantly, an improvement in the alpha angle on the latest radiographs, compared with the immediate post-operative ones, was noted.76 Despite some weaknesses, this study suggests that osseous remodelling and resorption continues for up to two years after femoral osteochondroplasty.
Recommendations
The burr should be handled gently during femoral osteochondroplasty to avoid creating bony indentations that may act as stress risers.
Post-operative instructions should include partial weight-bearing (50%) for six weeks.
A bone mineral density scan may be considered during pre-operative assessment in patients with suspected osteopenia or frank osteoporosis.73
Treatment of FAI: instability
Instability (subluxation or frank dislocation) is attributed to intra-operative compromise of one or more passive stabilisers of the joint (anterior capsule and iliofemoral ligament, labrum, acetabular osseous rim) during excessive rim osteoplasty for treatment of pincer impingement, a wide capsulotomy or aggressive labrectomy. The ligamentum teres has also been implicated in dysplastic hips,77 in which preservation of the labrum and avoidance of rim trimming, if the centre-edge angle is between 20° and 25°,55 are of utmost importance for the stability and longevity of the joint.55,78,79
Instability is rare, and the few reported cases share several features: gender (all female), a narrow age range (39 to 52 years, albeit unreported in one case19), early occurrence (immediately or within a few weeks), direction (all anterior) and the need for further surgery.19,55,77,78,80
Ito et al81 demonstrated in cadavers the biomechanical importance of the proximal capsule and the zona orbicularis to stability, the latter being described as a “locking ring” around the femoral neck, offering resistance to separation. We therefore recommend sparing the zona orbicularis during capsular dissection in the peripheral compartment. If there is concern or predisposing factors for instability, the anterior capsule, including the iliofemoral ligament, should be repaired at the end of the procedure.55,77,80
Recommendations
Risk factors for post-operative instability, including a centre-edge angle ≤ 25°, primary hyperlaxity, supraphysiological range of movement (e.g. gymnasts) or previous traumatic instability episodes, must be identified pre-operatively.
A centre-edge angle ≤ 20° is an absolute contraindication for acetabular rim trimming.
In order to minimise capsular dissection in patients with demonstrable capsular laxity or otherwise at risk for instability, the peripheral compartment should not be accessed through the central compartment, unless the capsule can be repaired at the end of the procedure.
Capsular dissection in the peripheral compartment should spare the zona orbicularis. If divided, the iliofemoral ligament should be repaired.
Treatment of FAI: heterotopic ossification
Heterotopic ossification (HO) after hip arthroscopy was largely unknown apart from occasional reports.6,17,82 The incidence of this complication appears to have increased as a result of arthroscopic techniques developed for treatment of FAI. It is theorised that surgical trauma to the gluteal muscles and the bone debris generated during osteoplasty might trigger the formation of new bone.48
Larson and Giveans83 reported a 6% rate of HO in 96 patients (100 hips) treated for FAI, with one patient suffering from significant restriction of movement secondary to ossification of the iliopsoas tendon that resolved by one year. An incidence of 1.6% in 300 cases of hip arthroscopy for FAI has been reported, with no post-operative prophylaxis against HO.84
Bedi et al85 studied 616 patients (616 hips) treated arthroscopically for FAI, internal snapping hip syndrome and disorders of the peritrochanteric space. The incidence of HO was 4.7% (n = 29; 21 men and eight women) at a mean of 13.2 months; seven patients required revision surgery to excise the HO. Two protocols were compared for prevention of HO: 1) 30 days of naproxen administration, and 2) four days of indomethacin, followed by 30 days of naproxen. Patients on naproxen-only developed HO more often (8.3% vs 1.8%) and were 4.36 times (95% CI 1.72 to 10.97) more likely to develop HO (p < 0.05): the authors concluded that indomethacin was effective prophylaxis for HO.
HO after hip arthroscopy may be expected to be mild, causing little functional compromise (Fig. 7). The literature suggests that at least a thorough washout of the joint would be recommended as prophylaxis against HO in femoral osteochondroplasty or acetabular rim trimming, but also following work on other osseous structures.86 Pharmacological prophylaxis is presently at the surgeon’s discretion.
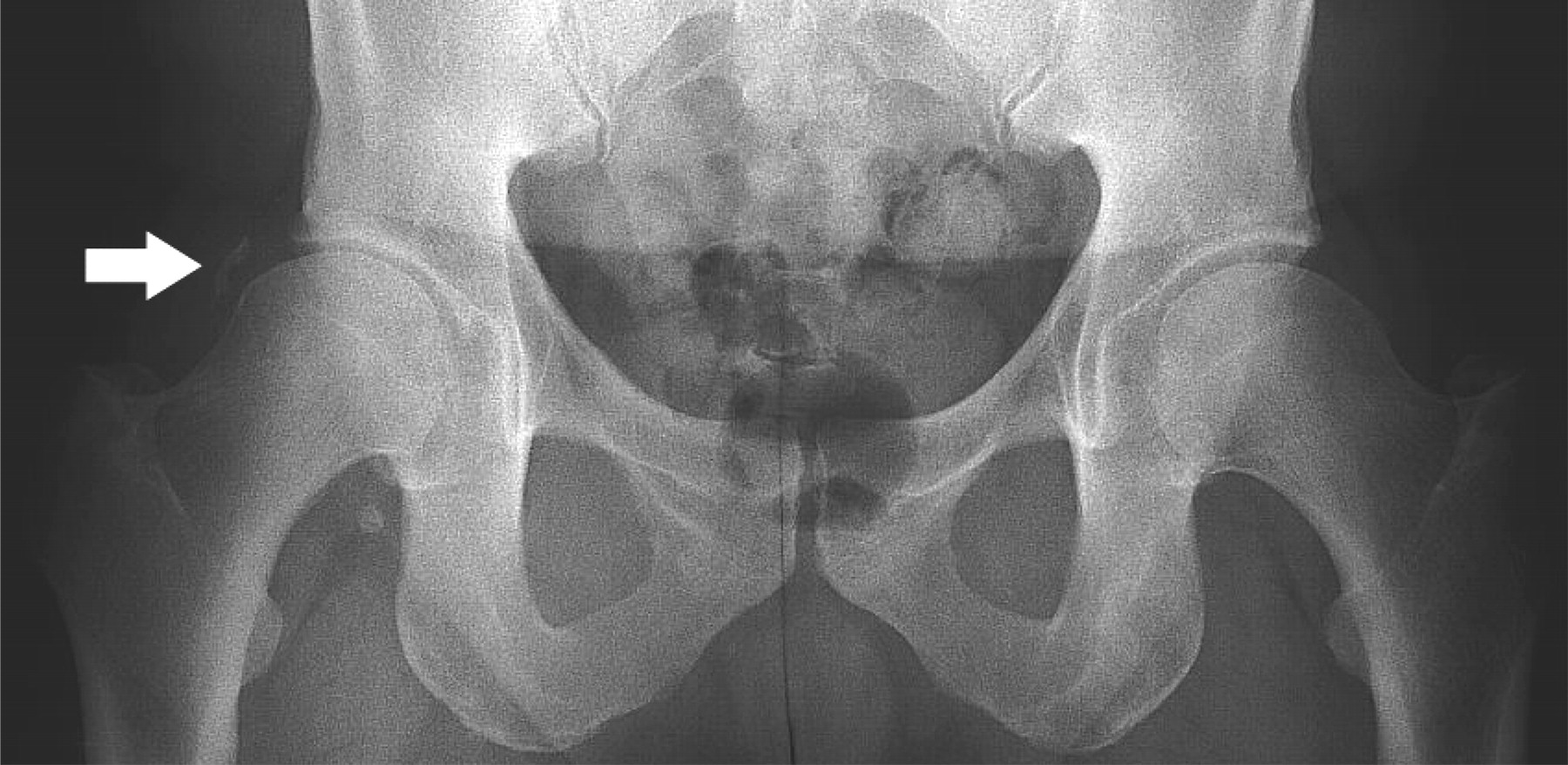
Fig. 7
Anteroposterior standing pelvic radiograph of a 52-year-old man showing mild joint space narrowing and minor heterotopic calcification (white arrow) of the right hip, after two arthroscopies of that joint with no post-operative prophylaxis given for heterotopic ossification.
Recommendations
The joint should be washed out at the end of procedures that generate bony debris.
In these cases, pharmacological prophylaxis (indomethacin (75 mg daily for four days) followed by naproxen (500 mg twice daily for 30 days)) should be administered, unless contraindicated.
If HO appears on a post-operative radiograph, follow-up (range of movement and imaging) should be continued for up to 12 months.
Treatment of FAI: inadequate osseous reshaping
Inadequate reshaping of the deformities is a newly recognised complication affecting outcome and emerging in studies of revision cases. In a series of 37 patients investigating the causes and outcomes of revision hip arthroscopy, 36 (97%) had radiological evidence of bony impingement either inadequately or not addressed.87 Another series found a 79% (19 of 24) rate of inadequate or absent osseous reshaping.11 Addressing the underlying bony pathoanatomy is a requisite for successful outcomes in FAI surgery.88
Thorough knowledge of the anatomy and surgical technique, and careful pre-operative planning to define the location and extent of bony resection are required. To this end, three-dimensional (3D) CT and MR arthrography are the best imaging modalities available. Using an image intensifier pre- and intra-operatively in planning and confirming adequacy of resection is recommended.72,89 The accuracy of osseous resection has been linked to surgical experience, based on improved outcomes assessed by the NonArthritic Hip Score.90
Recommendations
Pre-operative identification of the osseous lesions, ideally using 3D CT, helps planning and facilitates surgery.
The osseous deformity should be exposed adequately prior to resection.
The adequacy of bony resection may be confirmed by intra-operative fluoroscopy in multiple planes and dynamic testing in the impingement position.
Treatment of FAI: suture cut-through during labral repair
Repairs of labral tears of the hip using knotless suture anchors are now common. The suture may pass through the labral substance in a vertical mattress configuration, or around the labrum as a cinch stitch.91,92 During passage of the suture through the labrum or in cases of excessive tightening, there is a risk of the suture cutting through the labrum (Fig. 8).55 This may have serious biomechanical consequences, as it leads to sectioning of some or all of the circumferential fibres of the labrum, disrupting the associated hoop stresses.93
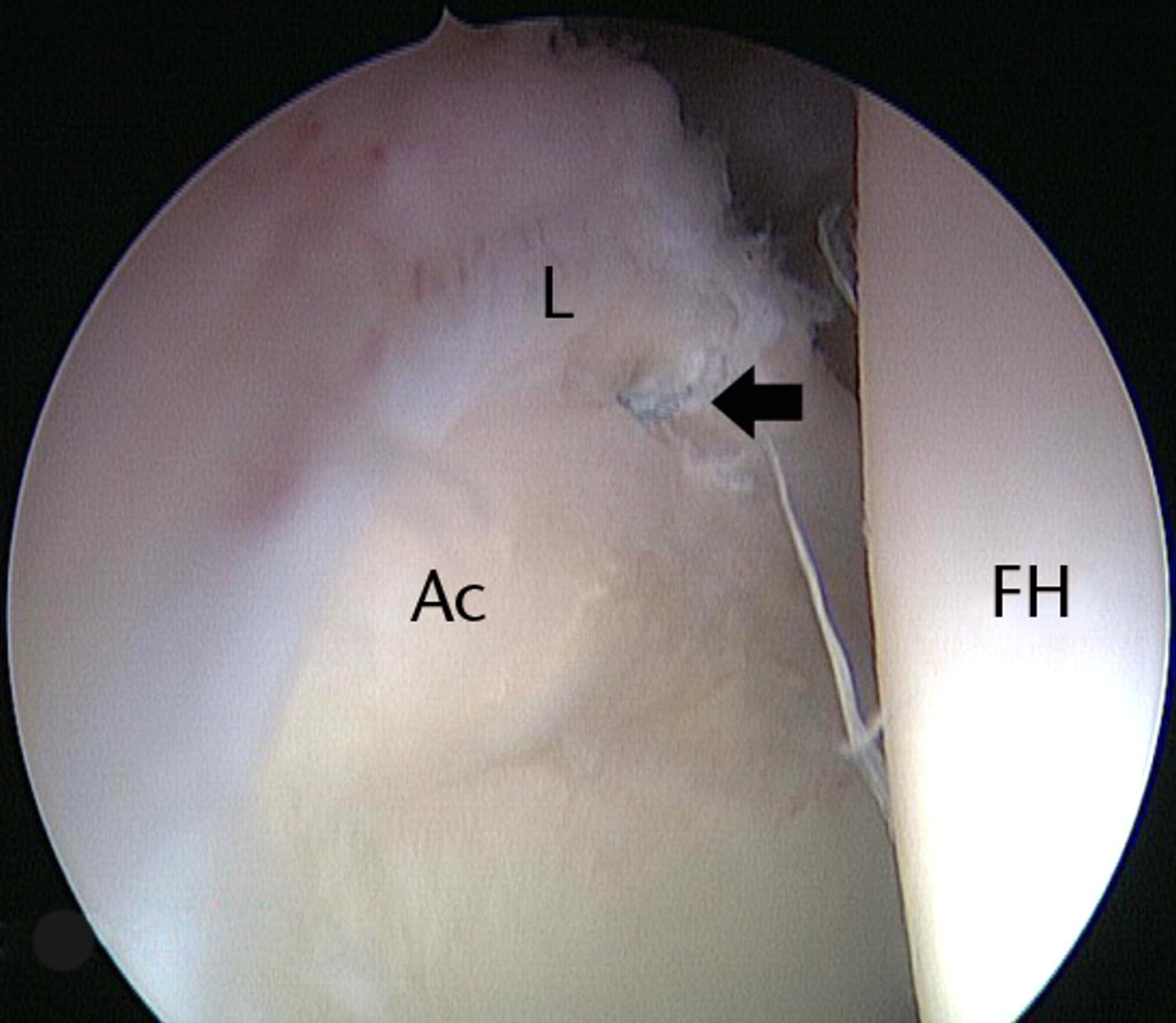
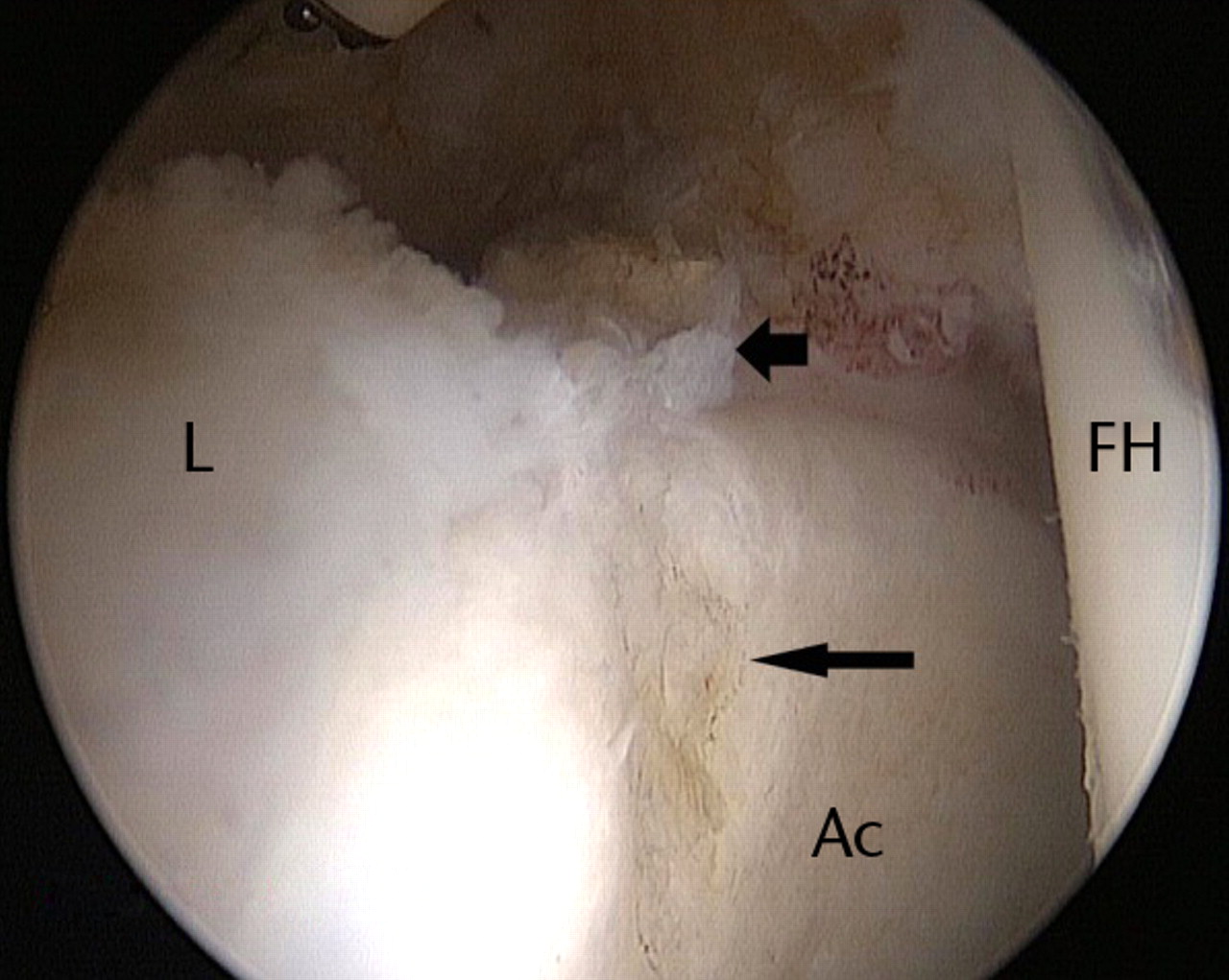
Figs. 8a - 8b
Figure 8a – arthroscopic image of a successful labral repair with use of the vertical mattress technique leaving the articular edge of the labrum free, with the suture barely visible (arrow). Figure 8b – arthroscopic image after an unsuccessful labral repair (cinch stitch technique) in which the suture cut through the labrum, showing the final appearance of debridement of the anterosuperior labrum (short arrow). Acetabular chondroplasty was also performed in that case (long arrow) (L, labrum; FH, femoral head; Ac, acetabulum).
A cut-through is more likely with the vertical mattress technique as the suture is looped around less labral tissue, leading some authors to recommend the cinch stitch technique.55 In turn, this has been criticised for potentially everting the labrum and not restoring its normal triangular cross-section and labral seal function,92 although the latter is debated.94
Recommendations
During labral repair, over-tightening of sutures must be avoided.
The cinch stitch technique is preferable when the labrum appears thin and/or friable.
Treatment of FAI: adhesions
After hip arthroscopy, adhesions tend to develop between the capsular side of the labrum and the capsule (Fig. 9), although they have also been described in the peripheral compartment between the femoral neck and the capsule after open femoral osteochondroplasty.30
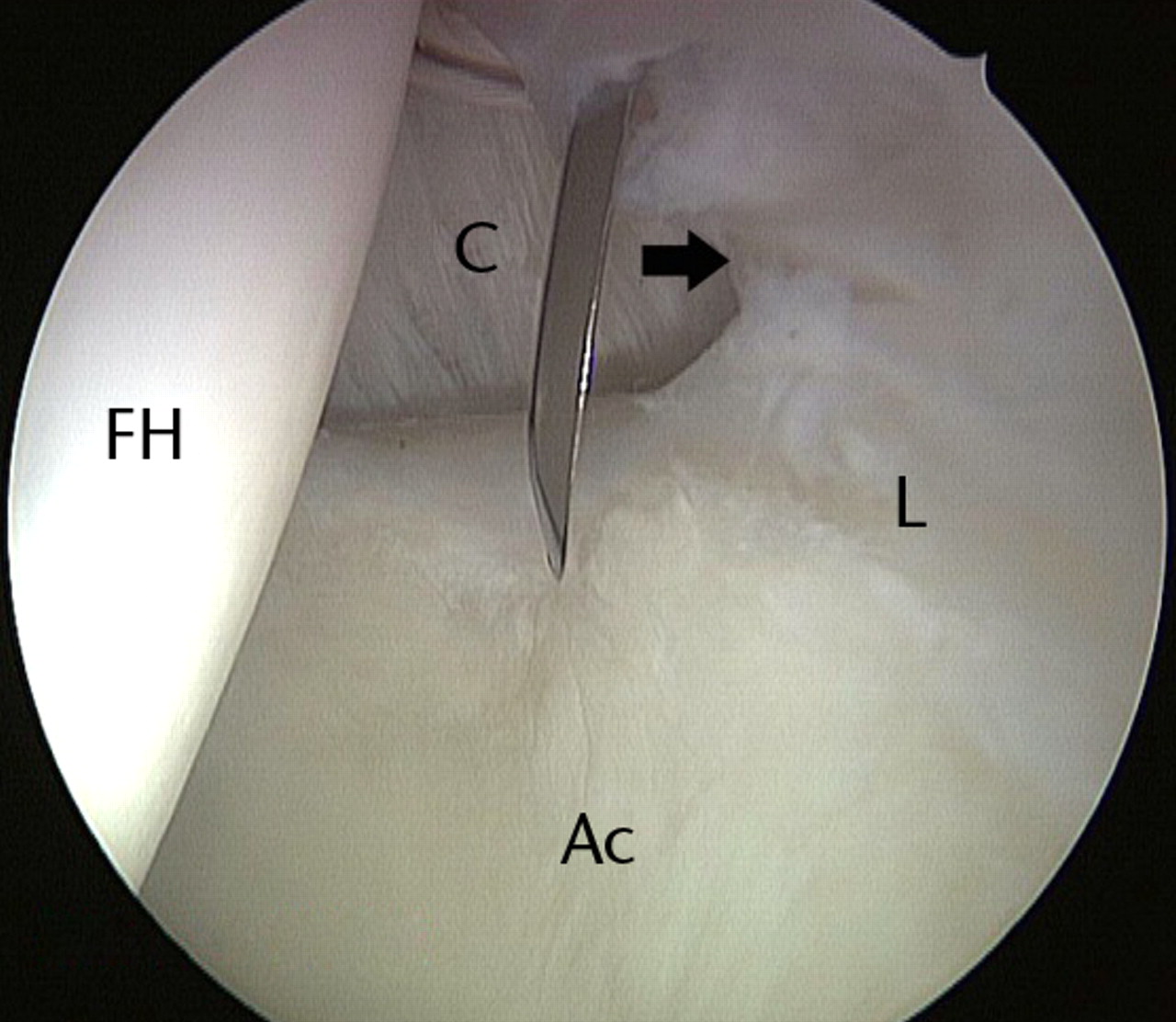
Figs. 9a - 9c
Arthroscopic images of the left hip of a 36-year-old woman who had a previous hip arthroscopy three years earlier, showing a) capsulolabral adhesions (arrow) in the area of the perilabral sulcus corresponding to the previous surgical intervention, in contrast to the normal capsule seen further anteriorly, b) removal of the adhesions, and c) chondroplasty with labral repair using a suture anchor. Symptoms improved as early as eight weeks post-operatively (FH, femoral head; Ac, acetabulum; L, labrum; C, capsule).
Adhesions as a cause of pain should be considered after any hip arthroscopy. Treatment of FAI often involves capsular dissection in the area of the perilabral sulcus; although one may speculate that adhesions occur more often after arthroscopic surgery for FAI than other indications, this is unproven. Adhesions are thought to cause symptoms by impairing the sealing function of the labrum or impinging against it.95 Patients complain of groin pain and demonstrate restricted flexion and rotation, with a positive impingement sign. MR arthrography is the benchmark diagnostic procedure (Fig. 10).95
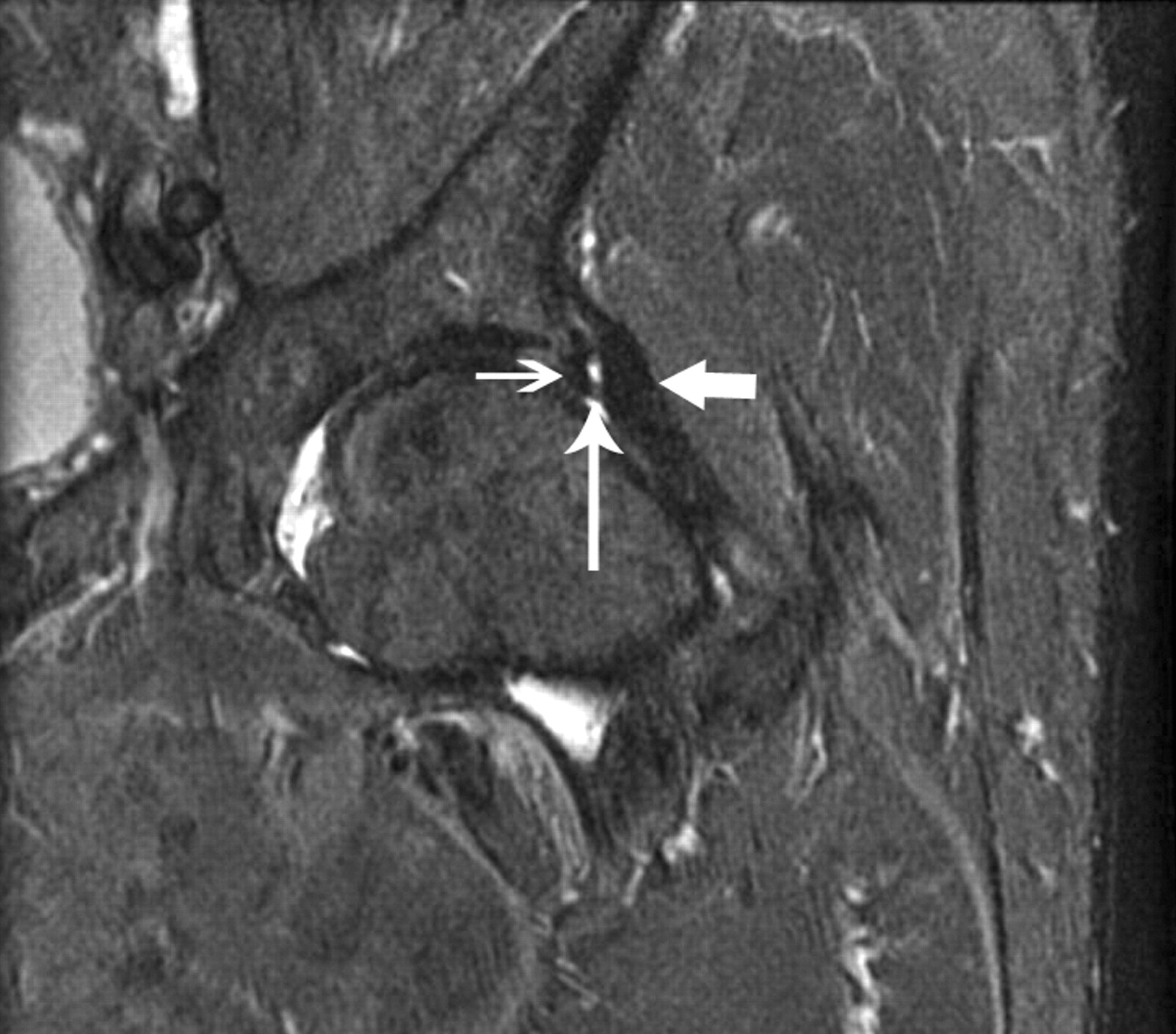
Fig. 10
Magnetic resonance arthrographic appearance (STIR sequence) of a left hip, 15 months following arthroscopic labral repair. The presence of adhesions (vertical arrow) is noted between the labrum (thin horizontal arrow) and the capsule (thick horizontal arrow).
The pathophysiology of adhesions after hip arthroscopy has not been studied in detail, but early post-operative movement is considered the best prevention.95,96 Persistent, symptomatic adhesions can be removed arthroscopically using an RF ablation probe and/or shaver, which was required in 22 of 37 patients (59%) undergoing revision hip arthroscopy.87 However, another series of 24 revision hip arthroscopies did not feature any adhesiolysis,11 highlighting the other reasons to be considered in a persistently painful arthroscoped hip.
The density of adhesions after open surgery for FAI can make arthroscopic adhesiolysis more technically demanding. Krueger et al30 reported symptomatic improvement in 13 of 16 patients (81%) with prior open surgical dislocation of the hip. In two patients, access to the central compartment proved impossible due to excessive scarring of the joint capsule. In this setting, releasing the adhesions in the peripheral compartment first has been advocated.95
In our experience, painful scarring may also develop in extra-articular hip endoscopy following release of the iliotibial band (ITB) and excision of the trochanteric bursa, with scar tissue building up on the undersurface of the ITB, tethering it to the greater trochanter. There are no relevant data in the literature, but we have had good results in two occasions with repeat cruciform release of the iliotibial band and adhesiolysis (Fig. 11).
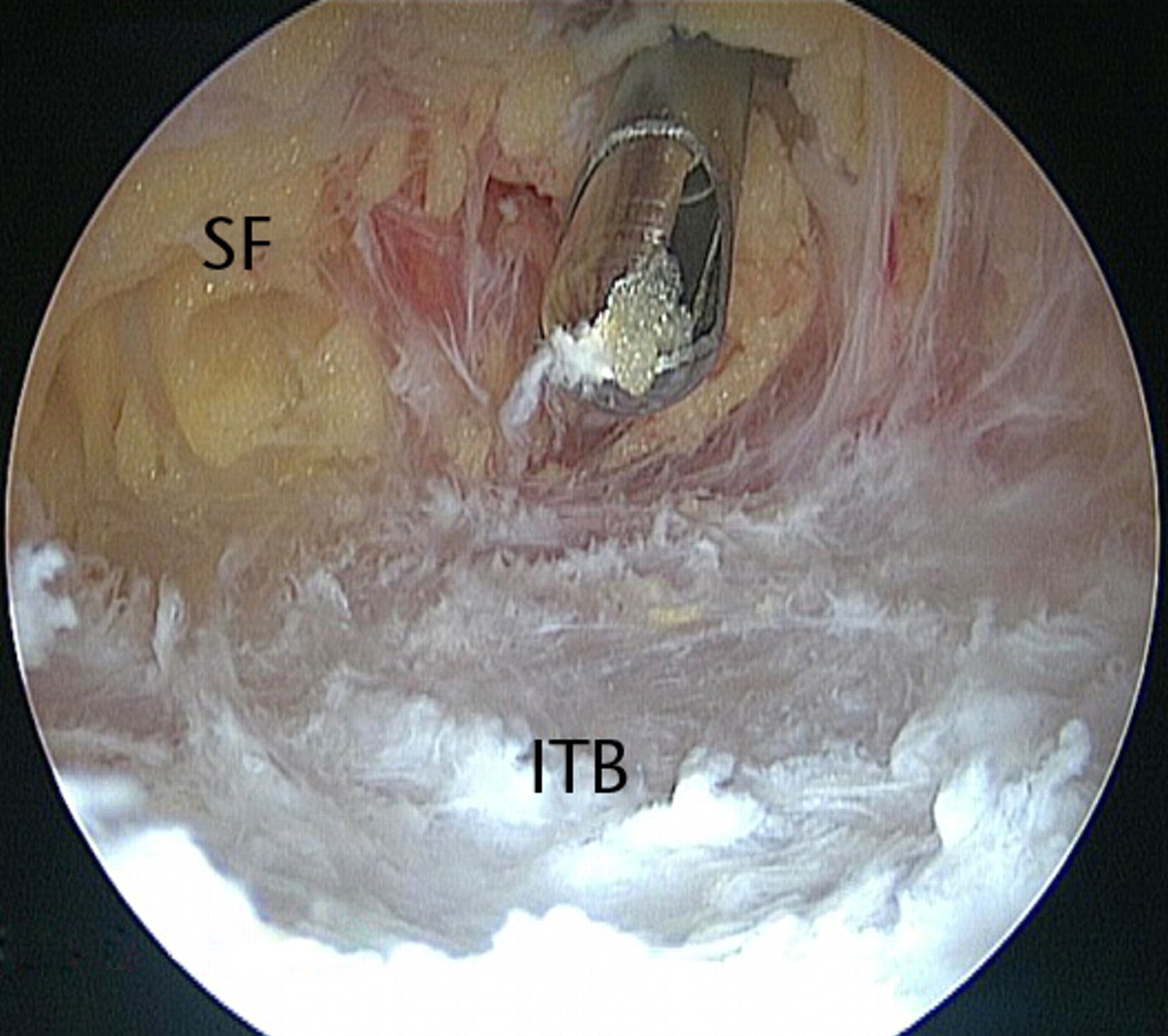
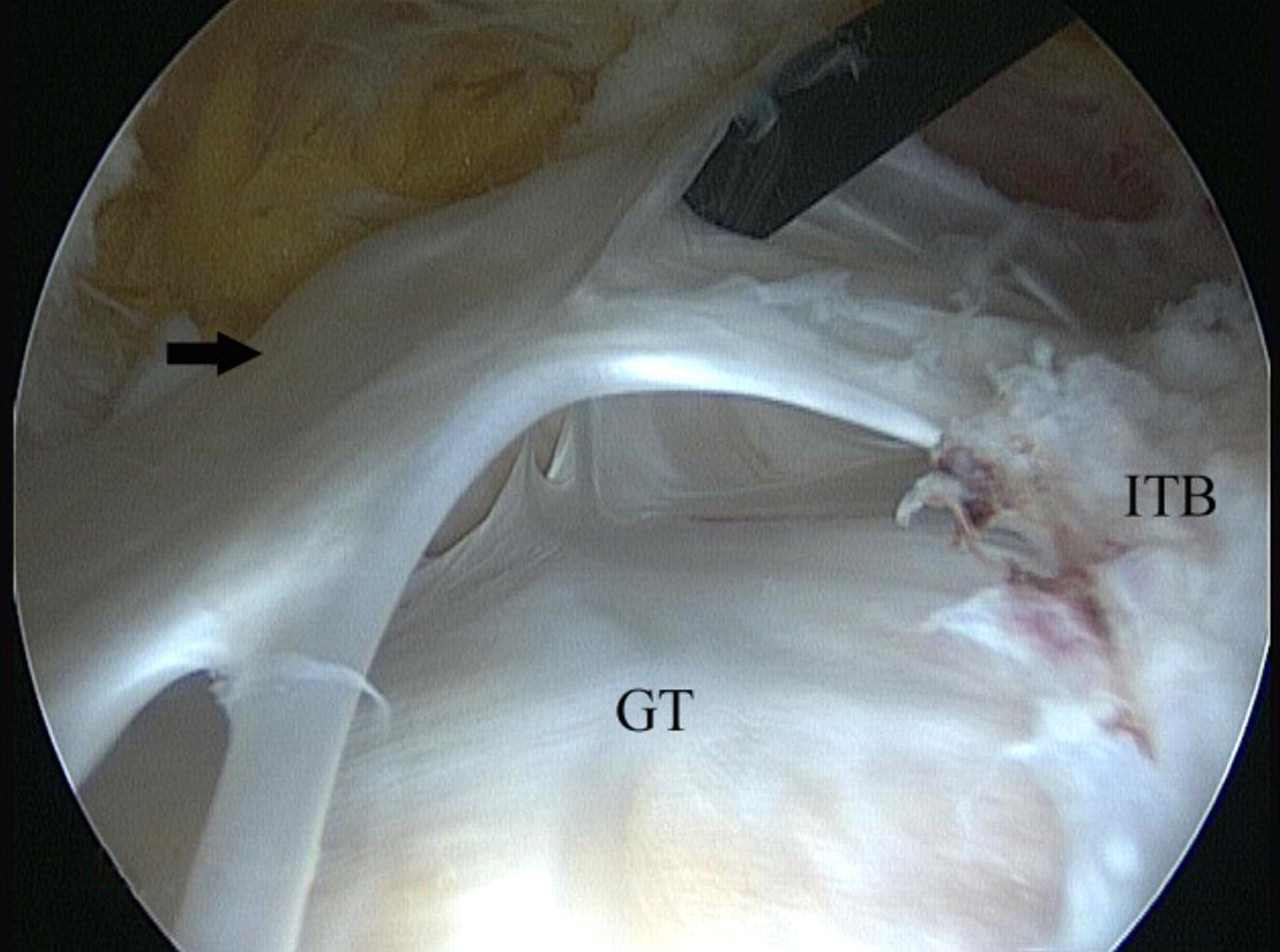
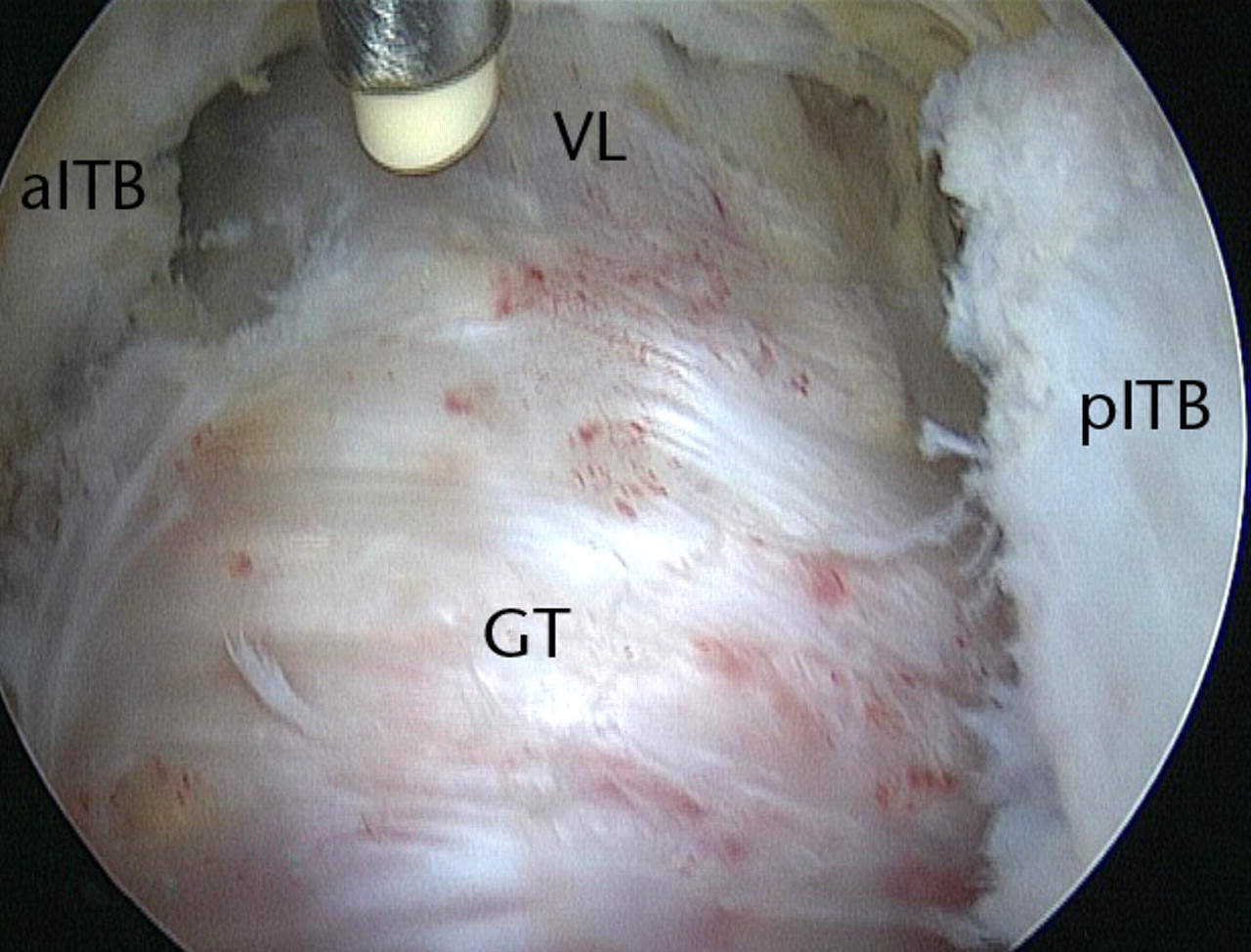
Figs. 11a - 11c
Arthroscopic images of the left hip of a 64-year-old woman with persistent pain following arthroscopic release of the iliotibial band (ITB) and excision of the trochanteric bursa. A revision endoscopy (a) revealed that the ITB flaps had healed back together. Upon opening of the ITB, significant adhesions (arrow) were found to have formed in the lateral compartment (b), tethering the ITB to the greater trochanter. After adhesiolysis and release of the ITB as distal as the origin of the vastus lateralis (c), there were marked improvements in symptoms, and the procedure was repeated on the right hip after seven months, with similar success (SF, subcutaneous fat; GT, greater trochanter; VL, vastus lateralis; aITB/pITB, anterior/posterior flap of the iliotibial band).
Recommendations
Continuous passive movement is helpful immediately post-operatively.
Post-operative range of movement exercises should be initiated as soon as pain allows. Stationary bicycles without resistance are ideal.
Arthroscopy after hip replacement surgery
Hip arthroscopy has become a valuable diagnostic and therapeutic tool for the management of patients after hip replacement.97-99 In the presence of a prosthetic joint, arthroscopic surgery is usually performed in the peripheral compartment only,99 avoiding the need for traction and minimising risks. No complications have been reported in two series of 14 patients (16 hips) and 24 patients (24 hips), respectively.98,99
Pain caused by an impinging iliopsoas tendon after hip replacement is treatable by arthroscopy,99 although posterior dislocation of the prosthetic joint after this procedure has been reported.100 Tenotomy of the iliopsoas may deprive the joint of an important dynamic stabiliser, which resists posterior translation of the prosthetic head. The presence of a retroverted cup and the previous use of a posterior surgical approach will accentuate such a destabilisation, and patients should be forewarned accordingly.
Recommendations
Post-operative “hip precautions” against dislocation may be useful when releasing the iliopsoas arthroscopically in the presence of a stemmed hip replacement.
Hip arthroscopy in children
Complications of hip arthroscopy in children are infrequent and of similar type to those seen in adults.50,57,101 In 54 arthroscopies performed in 42 patients aged ≤ 18 years, pudendal nerve palsy (n = 3), guide wire breakage (n = 1) and recurrent labral tears (n = 3) were reported.57 In a larger series from the same institution (218 arthroscopies in 175 patients), complications included transient pudendal nerve palsy (n = 2), instrument breakage (n = 1) and one case of suture abscess, with a complication rate of 1.8%.50
Asymptomatic HO was noted in a 13-year-old boy after successful arthroscopic resection of a malunited avulsion fracture of the anteroinferior iliac spine, coupled with rim trimming and labral reattachment.86 Surgery also involved a femoral osteochondroplasty, including part of the proximal femoral physis, with no adverse sequelae noted at 18 months’ follow-up.86 The development of radiological changes consistent with AVN in very young children undergoing hip arthroscopy for DDH,62,63 and the questionable link of this complication to the arthroscopic procedure itself,63 have been mentioned before.
Hip arthroscopy in children is technically demanding, due to small body size, variable anatomy and underlying pathologies and the possible history of previous surgeries.102 The amount of traction and the threshold of pressure to minimise extravasation have not been investigated in children. Careful patient positioning is paramount.102 Children operated on for femoral fractures are susceptible to traction-related nerve injuries.15 The foot must be well-padded prior to use of the foot holder to avoid undue pressure to the skin and nerves,103 although manual traction alone may be needed in very young children with hip dysplasia.62,63 Arthroscopic portals may have to be modified and smaller instrumentation used. Parents must be informed that, depending on the primary condition, hip arthroscopy may not be therapeutic and further operations may be necessary (most commonly osteotomies for dysplasia).102
Recommendations
Paediatric hip arthroscopy should only be performed by surgeons experienced in the specific technical challenges.
Rare complications
In a series of 35 hip arthroscopies of the peripheral compartment performed without traction, ten partial tears of the anterior synovial fold and one inadvertent detachment of an osteophyte occurred.34 Chronic regional pain syndrome has been described,104 but should constitute a diagnosis of exclusion. Trochanteric bursitis has been reported weeks after arthroscopy in one patient.5 This may have been due to repeated punctures of the bursa with the arthroscopic needle or altered gait biomechanics.
Conclusions: the importance of the learning curve
The low complication rates cited after hip arthroscopy are frequently derived from large series and experienced surgeons, and higher rates have been described.7,12 In one large series, complication rates were unrelated to learning curves,5 although other authors have reported fewer complications,6,7,12,57,90 shorter operating times and improved outcomes and patient satisfaction with experience.90
A learning curve of 30 cases has been suggested,90 although this should be interpreted cautiously. We believe it is the minimum number of hip arthroscopies a surgeon has to perform to avoid basic complications associated with patient positioning and access into the joint. However, more experience and confidence will result in surgeons performing increasingly complex cases, with the risk of different complications.19
Most complications of hip arthroscopy are minor or transient but serious complications do occur. Some have probably gone unreported. Any surgeon wishing to embark on hip arthroscopy should receive appropriate education in this technique, as requisites for a successful outcome include immaculate surgical technique, appropriate instrumentation and adherence to advice from experienced colleagues.6 To those, we add the critical role of patient selection. The increasing use, and lack of abuse, of this surgical technique will hopefully make it as common as arthroscopy of other joints.
1 Ganz R , ParviziJ, BeckM, et al.Femoroacetabular impingement: a cause for osteoarthritis of the hip. Clin Orthop Relat Res2003;417:112–120.CrossrefPubMed Google Scholar
2 McCarthy JC . Hip arthroscopy: applications and technique. J Am Acad Orthop Surg1995;3:115–122.CrossrefPubMed Google Scholar
3 Byrd JW . Hip arthroscopy: surgical indications. Arthroscopy2006;22:1260–1262.CrossrefPubMed Google Scholar
4 Diulus CA , KrebsVE, HannaG, BarsoumWK. Hip arthroscopy technique and indications. J Arthroplasty2006;21(Suppl):68–73.CrossrefPubMed Google Scholar
5 Griffin DR , VillarRN. Complications of arthroscopy of the hip. J Bone Joint Surg [Br]1999;81-B:604–606. Google Scholar
6 Sampson TG . Complications of hip arthroscopy. Tech Orthop2005;20:63–66.PubMed Google Scholar
7 Funke EL , MunzingerU. Complications in hip arthroscopy. Arthroscopy1996;12:156–159. Google Scholar
8 Clarke MT , AroraA, VillarRN. Hip arthroscopy: complications in 1054 cases. Clin Orthop Relat Res2003;406:84–88.CrossrefPubMed Google Scholar
9 Smart LR , OetgenM, NoonanB, MedveckyM. Beginning hip arthroscopy: indications, positioning, portals, basic techniques, and complications. Arthroscopy2007;23:1348–1353.CrossrefPubMed Google Scholar
10 Simpson J , SadriH, VillarR. Hip arthroscopy technique and complications. Orthop Traumatol Surg Res2010;96(Suppl):S68–S76.CrossrefPubMed Google Scholar
11 Heyworth BE , ShindleMK, VoosJE, RudzkiJR, KellyBT. Radiologic and intraoperative findings in revision hip arthroscopy. Arthroscopy2007;23:1295–1302.CrossrefPubMed Google Scholar
12 Lo YP , ChanYS, LienLC, et al.Complications of hip arthroscopy: analysis of seventy three cases. Chang Gung Med J2006;29:86–92.PubMed Google Scholar
13 Farjo LA , GlickJM, SampsonTG. Hip arthroscopy for acetabular labral tears. Arthroscopy1999;15:132–137.CrossrefPubMed Google Scholar
14 Byrd JW . Hip arthroscopy. J Am Acad Orthop Surg2006;14:433–444.CrossrefPubMed Google Scholar
15 Flierl MA , StahelPF, HakDJ, MorganSJ, SmithWR. Traction table-related complications in orthopaedic surgery. J Am Acad Orthop Surg2010;18:668–675.CrossrefPubMed Google Scholar
16 Sadri H. Complex therapeutic hip arthroscopy with the use of a femoral distractor. In: Sekiya JK, Safran MR, Ranawat AS, Leunig M, eds. Techniques in hip arthroscopy and joint preservation surgery. Philadelphia: Elsevier Saunders, 2011:113–120. Google Scholar
17 Gedouin JE , MayO, BoninN, et al.Assessment of arthroscopic management of femoroacetabular impingement: a prospective multicenter study. Orthop Traumatol Surg Res2010;96(Suppl):S59–S67. Google Scholar
18 Glick JM , SampsonTG, GordonRB, BehrJT, SchmidtE. Hip arthroscopy by the lateral approach. Arthroscopy1987;3:4–12.PubMed Google Scholar
19 Souza BG , DaniWS, HondaEK, et al.Do complications in hip arthroscopy change with experience?Arthroscopy2010;26:1053–1057.CrossrefPubMed Google Scholar
20 Eriksson E , ArvidssonI, ArvidssonH. Diagnostic and operative arthroscopy of the hip. Orthopedics1986;9:169–176.CrossrefPubMed Google Scholar
21 McLaren AC , FergusonJH, MiniaciA. Crush syndrome associated with use of the fracture-table: a case report. J Bone Joint Surg [Am]1987;69-A:1447–1449. Google Scholar
22 Coelho RF , GomesCM, SakakiMH, et al.Genitoperineal injuries associated with the use of an orthopedic table with a perineal posttraction. J Trauma2008;65:820–823.CrossrefPubMed Google Scholar
23 Brumback RJ , EllisonTS, MolliganH, et al.Pudendal nerve palsy complicating intramedullary nailing of the femur. J Bone Joint Surg [Am]1992;74-A:1450–1455.PubMed Google Scholar
24 Kruger DM , KaynerDC, HankinFM, et al.Traction force profiles associated with the use of a fracture table: a preliminary report. J Orthop Trauma1990;4:283–286.CrossrefPubMed Google Scholar
25 Toolan BC , KovalKJ, KummerFJ, GoldsmithME, ZuckermanJD. Effects of supine positioning and fracture post placement on the perineal countertraction force in awake volunteers. J Orthop Trauma1995;9:164–170.CrossrefPubMed Google Scholar
26 Merrell G , MedveckyM, DaigneaultJ, JoklP. Hip arthroscopy without a perineal post: a safer technique for hip distraction. Arthroscopy2007;23:107–101.CrossrefPubMed Google Scholar
27 McCarthy JC , MasonJB, LeeJA. Hip arthroscopy in the lateral position. Op Tech Sports Med2002;10:196–199. Google Scholar
28 Alaia MJ , ZuskovA, DavidovitchRI. Contralateral deep venous thrombosis after hip arthroscopy. Orthopedics2011;34:674–677.CrossrefPubMed Google Scholar
29 Byrd JW , ChernKY. Traction versus distension for distraction of the joint during hip arthroscopy. Arthroscopy1997;13:346–349.CrossrefPubMed Google Scholar
30 Krueger A , LeunigM, SiebenrockKA, BeckM. Hip arthroscopy after previous surgical hip dislocation for femoroacetabular impingement. Arthroscopy2007;23:1285–1289.CrossrefPubMed Google Scholar
31 Said HG , SteimerO, KohnD, DienstM. Vascular obstruction at the level of the ankle joint as a complication of hip arthroscopy. Arthroscopy2011;27:1594–1596.CrossrefPubMed Google Scholar
32 Ilizaliturri VM . Complications of arthroscopic femoroacetabular impingement treatment: a review. Clin Orthop Relat Res2009;467:760–768.CrossrefPubMed Google Scholar
33 Byrd JW . Avoiding the labrum in hip arthroscopy. Arthroscopy2000;16:770–773.CrossrefPubMed Google Scholar
34 Dienst M , GoddeS, SeilR, HammerD, KohnD. Hip arthroscopy without traction: in vivo anatomy of the peripheral hip joint cavity. Arthroscopy2001;17:924–931.CrossrefPubMed Google Scholar
35 McCarthy JC , LeeJA. Hip arthroscopy: indications, outcomes, and complications. Instr Course Lect2006;55:301–308.PubMed Google Scholar
36 Ilizaliturri VM, Jr., Camacho-Galindo J, Ugalde HG, Evia Ramirez AN. Paper #13: Cartilage injury caused by hip scope. Procs International Society for Hip Arthroscopy Annual Scientific Meeting. Paris. 2011. Google Scholar
37 Badylak JS , KeeneJS. Do iatrogenic punctures of the labrum affect the clinical results of hip arthroscopy?Arthroscopy2011;27:761–767.CrossrefPubMed Google Scholar
38 Dienst M , SeilR, KohnDM. Safe arthroscopic access to the central compartment of the hip. Arthroscopy2005;21:1510–1514.CrossrefPubMed Google Scholar
39 Haupt U , VölkleD, WaldherrC, BeckM. Intra- and retroperitoneal irrigation liquid after arthroscopy of the hip joint. Arthroscopy2008;24:966–968.CrossrefPubMed Google Scholar
40 Ladner B , NesterK, CascioB. Abdominal fluid extravasation during hip arthroscopy. Arthroscopy2010;26:131–135.CrossrefPubMed Google Scholar
41 Sharma A , SachdevH, GomillionM. Abdominal compartment syndrome during hip arthroscopy. Anaesthesia2009;64:567–569.CrossrefPubMed Google Scholar
42 Verma M , SekiyaJK. Intrathoracic fluid extravasation after hip arthroscopy. Arthroscopy2010;26(Suppl):S90–S94.CrossrefPubMed Google Scholar
43 Fowler J , OwensBD. Abdominal compartment syndrome after hip arthroscopy. Arthroscopy2010;26:128–130.CrossrefPubMed Google Scholar
44 Bartlett CS , DiFeliceGS, BulyRL, et al.Cardiac arrest as a result of intraabdominal extravasation of fluid during arthroscopic removal of a loose body from the hip joint of a patient with an acetabular fracture. J Orthop Trauma1998;12:294–299.CrossrefPubMed Google Scholar
45 Yamamoto Y , IdeT, OnoT, HamadaY. Usefulness of arthroscopic surgery in hip trauma cases. Arthroscopy2003;19:269–273.CrossrefPubMed Google Scholar
46 DiStefano VJ , KalmanVR, O'MalleyJS. Femoral nerve palsy after arthroscopic surgery with an infusion pump irrigation system: a report of three cases. Am J Orthop (Belle Mead NJ)1996;25:145–148. Google Scholar
47 Siegel MG . Irrigation fluid complications. Arthroscopy2010;26:576.CrossrefPubMed Google Scholar
48 Fabricant PD , MaakTG, CrossMB, KellyBT. Avoiding complications in hip arthroscopy. Op Tech Sports Med2011;19:108–113. Google Scholar
49 Stafford GH , MalviyaA, VillarRN. Fluid extravasation during hip arthroscopy. Hip Int2011;21:740–743.CrossrefPubMed Google Scholar
50 Nwachukwu BU , McFeelyED, NasreddineAY, et al.Complications of hip arthroscopy in children and adolescents. J Pediatr Orthop2011;31:227–231.CrossrefPubMed Google Scholar
51 Hawkins RB . Arthroscopy of the hip. Clin Orthop Relat Res1989;249:44–47.CrossrefPubMed Google Scholar
52 Bushnell BD , DahnersLE. Fatal pulmonary embolism in a polytraumatized patient following hip arthroscopy. Orthopedics2009;32:56.CrossrefPubMed Google Scholar
53 Salvo JP , TroxellCR, DugganDP. Incidence of venous thromboembolic disease following hip arthroscopy. Orthopedics2010;33:664.CrossrefPubMed Google Scholar
54 Clohisy JC , ZebalaLP, NeppleJJ, PashosG. Combined hip arthroscopy and limited open osteochondroplasty for anterior femoroacetabular impingement. J Bone Joint Surg [Am]2010;92-A:1697–1706.CrossrefPubMed Google Scholar
55 Matsuda DK . Acute iatrogenic dislocation following hip impingement arthroscopic surgery. Arthroscopy2009;25:400–404.CrossrefPubMed Google Scholar
56 No authors listed. General nitinol effects. www.memry.com/nitinol-iq/nitinol-fundamentals/nitinol-effects (date last accessed 10 April 2012). Google Scholar
57 Kocher MS , KimYJ, MillisMB, et al.Hip arthroscopy in children and adolescents. J Pediatr Orthop2005;25:680–686.CrossrefPubMed Google Scholar
58 Villar RN . Arthroscopic debridement of the hip: a minimally invasive approach to osteoarthritis. J Bone Joint Surg [Br]1991;73-B(Suppl):170–171. Google Scholar
59 Scher DL , BelmontPJ, OwensBD. Case report: osteonecrosis of the femoral head after hip arthroscopy. Clin Orthop Relat Res2010;468:3121–3125.CrossrefPubMed Google Scholar
60 Sener N , GogusA, AkmanS, HamzaogluA. Avascular necrosis of the femoral head after hip arthroscopy. Hip Int2011;21:623–626.CrossrefPubMed Google Scholar
61 Kalhor M , BeckM, HuffTW, GanzR. Capsular and pericapsular contributions to acetabular and femoral head perfusion. J Bone Joint Surg [Am]2009;91-A:409–418.CrossrefPubMed Google Scholar
62 McCarthy JJ , MacEwenGD. Hip arthroscopy for the treatment of children with hip dysplasia: a preliminary report. Orthopedics2007;30:262–264.CrossrefPubMed Google Scholar
63 Eberhardt O , FernandezFF, WirthT. Arthroscopic reduction of the dislocated hip in infants. J Bone Joint Surg [Br]2012;94-B:842–847.CrossrefPubMed Google Scholar
64 Rodeo SA , ForsterRA, WeilandAJ. Neurological complications due to arthroscopy. J Bone Joint Surg [Am]1993;75-A:917–926.CrossrefPubMed Google Scholar
65 Byrd JW , PappasJN, PedleyMJ. Hip arthroscopy: an anatomic study of portal placement and relationship to the extra-articular structures. Arthroscopy1995;11:418–423.CrossrefPubMed Google Scholar
66 Dorfmann H , BoyerT. Hip arthroscopy utilizing the supine position. Arthroscopy1996;12:264–267.CrossrefPubMed Google Scholar
67 Elsaidi GA , RuchDS, SchaeferWD, KuzmaK, SmithBP. Complications associated with traction on the hip during arthroscopy. J Bone Joint Surg [Br]2004;86-B:793–796.CrossrefPubMed Google Scholar
68 Robertson WJ , KellyBT. The safe zone for hip arthroscopy: a cadaveric assessment of central, peripheral, and lateral compartment portal placement. Arthroscopy2008;24:1019–1026.CrossrefPubMed Google Scholar
69 Bruno M , LonghinoV, SansoneV. A catastrophic complication of hip arthroscopy. Arthroscopy2011;27:1150–1152.CrossrefPubMed Google Scholar
70 Byrd JW , JonesKS. Prospective analysis of hip arthroscopy with 10-year followup. Clin Orthop Relat Res2010;468:741–746.CrossrefPubMed Google Scholar
71 Goulding K , BeaulePE, KimPR, FazekasA. Incidence of lateral femoral cutaneous nerve neuropraxia after anterior approach hip arthroplasty. Clin Orthop Relat Res2010;468:2397–2404.CrossrefPubMed Google Scholar
72 Larson CM , WulfCA. Intraoperative fluoroscopy for evaluation of bony resection during arthroscopic management of femoroacetabular impingement in the supine position. Arthroscopy2009;25:1183–1192.CrossrefPubMed Google Scholar
73 Mardones RM , GonzalezC, ChenQ, et al.Surgical treatment of femoroacetabular impingement: evaluation of the effect of the size of the resection. J Bone Joint Surg [Am]2005;87-A:273–279.CrossrefPubMed Google Scholar
74 Ayeni OR , BediA, LorichDG, KellyBT. Femoral neck fracture after arthroscopic management of femoroacetabular impingement: a case report. J Bone Joint Surg [Am]2011;93-A:47.CrossrefPubMed Google Scholar
75 Laude F , SarialiE, NogierA. Femoroacetabular impingement treatment using arthroscopy and anterior approach. Clin Orthop Relat Res2009;467:747–752.CrossrefPubMed Google Scholar
76 Nassif NA , PekmezciM, PashosG, SchoeneckerPL, ClohisyJC. Osseous remodeling after femoral head-neck junction osteochondroplasty. Clin Orthop Relat Res2010;468:511–518.CrossrefPubMed Google Scholar
77 Mei-Dan O , McConkeyMO, BrickM. Catastrophic failure of hip arthroscopy due to iatrogenic instability: can partial division of the ligamentum teres and iliofemoral ligament cause subluxation?Arthroscopy2012;28:440–445.CrossrefPubMed Google Scholar
78 Benali Y , KatthagenBD. Hip subluxation as a complication of arthroscopic debridement. Arthroscopy2009;25:405–407.CrossrefPubMed Google Scholar
79 Parvizi J , BicanO, BenderB, et al.Arthroscopy for labral tears in patients with developmental dysplasia of the hip: a cautionary note. J Arthroplasty2009;24:110–113.CrossrefPubMed Google Scholar
80 Ranawat AS , McClincyM, SekiyaJK. Anterior dislocation of the hip after arthroscopy in a patient with capsular laxity of the hip: a case report. J Bone Joint Surg [Am]2009;91-A:192–197. Google Scholar
81 Ito H , SongY, LindseyDP, SafranMR, GioriNJ. The proximal hip joint capsule and the zona orbicularis contribute to hip joint stability in distraction. J Orthop Res2009;27:989–995.CrossrefPubMed Google Scholar
82 Byrd JW , JonesKS. Arthroscopic management of femoroacetabular impingement in athletes. Am J Sports Med2011;39(Suppl):7S–13S.CrossrefPubMed Google Scholar
83 Larson CM , GiveansMR. Arthroscopic management of femoroacetabular impingement: early outcomes measures. Arthroscopy2008;24:540–546.CrossrefPubMed Google Scholar
84 Randelli F , PierannunziiL, BanciL, et al.Heterotopic ossifications after arthroscopic management of femoroacetabular impingement: the role of NSAID prophylaxis. J Orthop Traumatol2010;11:245–250.CrossrefPubMed Google Scholar
85 Bedi A , ZbedaRM, BuenoVF, et al.The incidence of heterotopic ossification after hip arthroscopy. Am J Sports Med2012;40:854–863.CrossrefPubMed Google Scholar
86 Matsuda DK , CalipusanCP. Adolescent femoroacetabular impingement from malunion of the anteroinferior iliac spine apophysis treated with arthroscopic spinoplasty. Orthopedics2012;35:460–463.CrossrefPubMed Google Scholar
87 Philippon MJ , SchenkerML, BriggsKK, et al.Revision hip arthroscopy. Am J Sports Med2007;35:1918–1921.CrossrefPubMed Google Scholar
88 May O , MatarWY, BeauléPE. Treatment of failed arthroscopic acetabular labral debridement by femoral chondro-osteoplasty: a case series of five patients. J Bone Joint Surg [Br]2007;89-B:595–598.CrossrefPubMed Google Scholar
89 Matsuda DK . Fluoroscopic templating technique for precision arthroscopic rim trimming. Arthroscopy2009;25:1175–1182.CrossrefPubMed Google Scholar
90 Konan S , RheeSJ, HaddadFS. Hip arthroscopy: analysis of a single surgeon’s learning experience. J Bone Joint Surg [Am]2011;93-A(Suppl 2):52–56. Google Scholar
91 Kelly BT , WeilandDE, SchenkerML, PhilipponMJ. Arthroscopic labral repair in the hip: surgical technique and review of the literature. Arthroscopy2005;21:1496–1504.CrossrefPubMed Google Scholar
92 Fry R , DombB. Labral base refixation in the hip: rationale and technique for an anatomic approach to labral repair. Arthroscopy2010;26(Suppl):S81–S89.CrossrefPubMed Google Scholar
93 Safran MR . The acetabular labrum: anatomic and functional characteristics and rationale for surgical intervention. J Am Acad Orthop Surg2010;18:338–345.CrossrefPubMed Google Scholar
94 Lertwanich P , EjnismanL, PhilipponMJ. Comments on “Labral base refixation in the hip: rationale and technique for an anatomic approach to labral repair”. Arthroscopy2011;27:303–304. Google Scholar
95 Beck M . Groin pain after open FAI surgery: the role of intraarticular adhesions. Clin Orthop Relat Res2009;467:769–774.CrossrefPubMed Google Scholar
96 Willimon SC , PhilipponMJ, BriggsKK. Risk factors for adhesions following hip arthroscopy. Arthroscopy2011;27(Suppl):50–51. Google Scholar
97 Khanduja V , VillarRN. The role of arthroscopy in resurfacing arthroplasty of the hip. Arthroscopy2008;24:122.CrossrefPubMed Google Scholar
98 McCarthy JC , JibodhSR, LeeJA. The role of arthroscopy in evaluation of painful hip arthroplasty. Clin Orthop Relat Res2009;467:174–180.CrossrefPubMed Google Scholar
99 Bajwa AS , VillarRN. Arthroscopy of the hip in patients following joint replacement. J Bone Joint Surg [Br]2011;93-B:890–896.CrossrefPubMed Google Scholar
100 Jones CW , BiantLC, FieldRE. Dislocation of a total hip arthroplasty following hip arthroscopy. Hip Int2009;19:396–398.CrossrefPubMed Google Scholar
101 Schindler A , LechevallierJJ, RaoNS, BowenJR. Diagnostic and therapeutic arthroscopy of the hip in children and adolescents: evaluation of results. J Pediatr Orthop1995;15:317–321.CrossrefPubMed Google Scholar
102 Jayakumar P , RamachandranM, YoumT, AchanP. Arthroscopy of the hip for paediatric and adolescent disorders: current concepts. J Bone Joint Surg [Br]2012;94-B:290–296.CrossrefPubMed Google Scholar
103 Roy DR . Arthroscopy of the hip in children and adolescents. J Child Orthop2009;3:89–100.CrossrefPubMed Google Scholar
104 Kim SJ , ChoiNH, KimHJ. Operative hip arthroscopy. Clin Orthop Relat Res1998;353:156–165. Google Scholar
Funding statement:
None declared
Author contributions:
A. V. Papavasiliou: Writing and researching the paper
N. V. Bardakos: Writing and researching the paper
ICMJE Conflict of Interest:
None declared
©2012 British Editorial Society of Bone and Joint Surgery. This is an open-access article distributed under the terms of the Creative Commons Attributions licence, which permits unrestricted use, distribution, and reproduction in any medium, but not for commercial gain, provided the original author and source are credited.
