




Abstract
Aims
Magnetically controlled growing rods (MCGR) have been gaining popularity in the management of early-onset scoliosis (EOS) over the past decade. We present our experience with the first 44 MCGR consecutive cases treated at our institution.
Methods
This is a retrospective review of consecutive cases of MCGR performed in our institution between 2012 and 2018. This cohort consisted of 44 children (25 females and 19 males), with a mean age of 7.9 years (3.7 to 13.6). There were 41 primary cases and three revisions from other rod systems. The majority (38 children) had dual rods. The group represents a mixed aetiology including idiopathic (20), neuromuscular (13), syndromic (9), and congenital (2). The mean follow-up was 4.1 years, with a minimum of two years. Nine children graduated to definitive fusion. We evaluated radiological parameters of deformity correction (Cobb angle), and spinal growth (T1-T12 and T1-S1 heights), as well as complications during the course of treatment.
Results
The mean Cobb angles pre-operatively, postoperatively, and at last follow-up were 70° (53 to 103), 35° (15 to 71) and 39° (15 to 65) respectively (p < 0.001). Further, there was a mean of 14° (-6 to 27) of additional Cobb angle correction upon graduation from MCGR to definitive fusion. Both T1-T12 and T1-S1 showed significant increase in heights of 27 mm and 45 mm respectively at last follow-up (p < 0.001). Ten children (23%) developed 18 complications requiring 21 unplanned operations. Independent risk factors for developing a complication were single rod constructs and previous revision surgery.
Conclusion
MCGR has the benefit of avoiding multiple surgeries, and is an effective tool in treatment of early-onset scoliosis. It also maintains the flexibility of the spine, allowing further correction at the time of definitive fusion.
Cite this article: Bone Joint Open 2020;1-7:405–414.
Introduction
Early onset scoliosis (EOS) remains one of the most challenging conditions to treat in paediatric orthopaedic surgery.1 Non-surgical management options (casting, bracing, or a combination of both) are usually employed as the first line of treatment. However, cases refractory to non-surgical management may require surgical intervention. The aims of surgery in early onset scoliosis are threefold: control the deformity, promote the development of chest and lungs and preserve the growth potential of the spine.2
The concept of growing rods has been used in the treatment of EOS since 1960s, when Harrington3 reported his technique of using a single rod and periodic lengthening procedures to distract the spine. In attempts to improve the outcomes of Harrington rod system, several authors modified it and reported on their results, including Moe et al,4 Klemme et al,5 Blakemore et al,6 and Mineiro and Weinstein.7 It was not until 2005 that Akbarnia et al8 published the first report on the use of dual growing rods, coined later with the name traditional growing rods (TGR).
Growing rods have since proved to be effective in the management of EOS.9 However, the invasive nature of the serial distraction procedures remained a significant drawback. Open distraction procedures require hospital admission with general anaesthetic, and return to operating theatre six- to nine-monthly, resulting in high procedure-related complication rates (up to 58%). There is also a potential increase of 24% in risk of complications per additional episode of surgery.10 The development of magnetic controlled growing rod (MCGR) systems was an attempt to overcome the obstacle of repeated lengthening surgical procedures and the resultant adverse medical and psychological effects on the children and their families.11 Over the past decade, multiple authors from various centres around the world have reported the results of their experiences. This has created a growing body of evidence on the outcomes of MCGR in the treatment of EOS.12
Our institution, a major tertiary referral centre, adopted the use of MCGR concept in January 2012. In this paper, we report our results, with a particular review of the effect of MCGR on deformity correction, spinal growth and complication rates.
Methods
We retrospectively reviewed all patients with early onset scoliosis who were treated at Alder Hey Children's Hospital, Liverpool, UK, with magnetic controlled growing rods (MAGEC growing rod system; NuVasive, San Diego, California, USA) with a minimum of two years of follow-up. These children were treated between January 2012 (our institution’s first case) and March 2018. A total of 44 patients (25 females and 19 males) were identified. Their mean age at time of surgery was 7.9 years (3.7 to 13.6). There was one patient aged 13.6 years at time of MGCR insertion; the remainder were aged 3.7 to 11 years of age. This child was originally planned for fusion. However, at the time of surgery, it was noticed that he had open growth plates, and hence decision was made to proceed with MCGRs. He had fusion 34 months later after having 11 clinic distractions. Children were followed up for a mean of 4.1 years (2 to 6). The follow-up endpoint was determined to be the last encounter with the treating team if patients are still undergoing distractions; or definitive fusion if they have reached that stage. Aetiological diagnosis included idiopathic (20), neuromuscular (13), syndromic (9) and congenital (2). There were three cases revised from other rod systems to MCGRs (two TGR and one Shilla system). The remaining 41 cases were primary procedures. Dual rods were used in 38 patients, while single rods were used in six. It is worth noting that the group of patients in whom single rods were used were in the beginning of our MCGR experience. At that time, single rod use was the standard practice. However, single rods were soon abandoned because of high incidence of complications reported from multiple centres.13,14 Subsequently, only dual rods were used in our unit. Patients’ characteristics are summarized in Table I.
Table I.
Patient characteristics.
| Variable | Mean (range) |
|---|---|
| Age (years) | 7.9 (3.7 to 13.6) |
| Sex | 25 females 18 males |
| Aetiology | 20 idiopathic 13 neuromuscular 9 syndromic 2 congenital |
| Primary/revision | 41 primary 3 revisions (2 TGR, 1 Shilla rods) |
| Rod configuration | 38 dual rods 6 single rod |
| Number of distractions per child | 11.3 (4 to 18) |
| Length of follow-up (years) | 4.1 (2 to 6) |
-
TGR, traditional growing rods.
Procedure
All procedures were performed by the three senior authors (JT, NTD, SM) in the standard manner. Proximal and distal foundation construct levels were identified with intra-operative fluoroscopy. Proximal and distal incisions allowed for insertion of proximal and distal anchors without violation of the intermediate section of the spine. Distally, pedicle screws were used, while either ribs or vertebrae were used as anchor points proximally. Rods were contoured then tunnelled sub-muscularly and connected to the anchors. Our unit has previously reported on the technique we use for rod insertion.15 On-table deformity correction was achieved. While exposure of the spine was kept to minimum, limited fusion at the sites of the instrumented foundation levels was facilitated by decortication. Intra-operative spinal cord monitoring was used throughout the procedure. Rod incremental distractions were performed at the outpatient clinics using a handheld external remote controller (ERC) at an average rate of 3 mm every three months. The distraction rate was calculated to follow the natural growth of the spine of an average of 1 mm/month, based on the tail-gating technique described by Dimeglio et al14 Radiographs and ultrasound scans were used to confirm and quantify the amount of distraction achieved. Patients had a mean of 11.3 distractions per patient (4 to 18).
Postoperative course was examined to identify the number of lengthening episodes, complications, revision surgery for any reason and finally, if patients graduated from MCGRs to definitive fusion. Pre- and postoperative radiographs were also evaluated. Pre-operative, immediate postoperative, and final Cobb angle measures were recorded. T1-T12 and T1-S1 spinal segments lengths were also measured to assess the effect of surgery on the growth of the spine. Lengths were measured on both coronal and sagittal views and the average of the two readings was documented pre-operatively and at final follow-up (Figures 1-2).
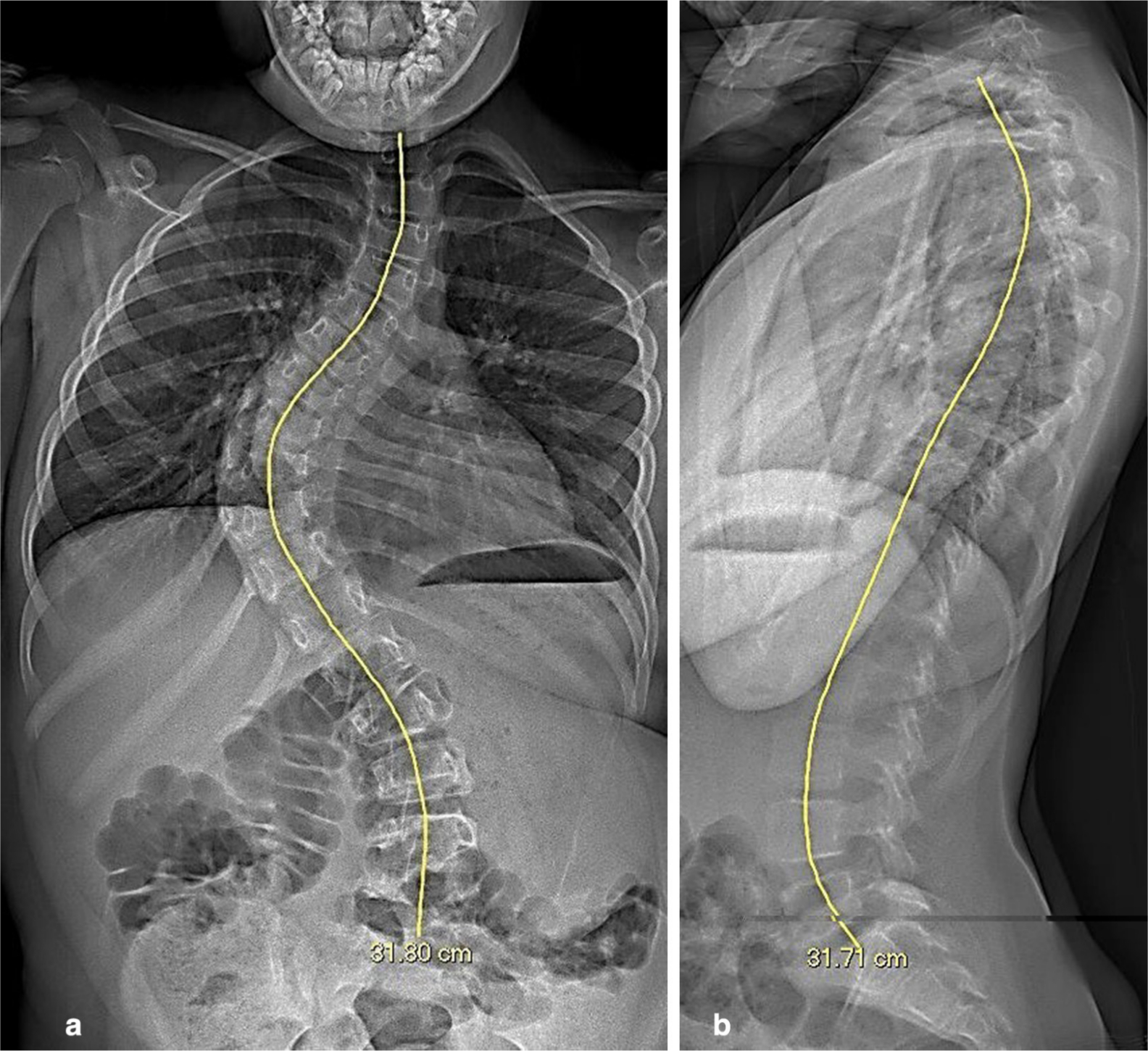
Fig. 1
a) Pre-operative coronal view radiograph with T1-S1 measurement. b) Pre-operative sagittal view radiograph with T1-S1 measurement.
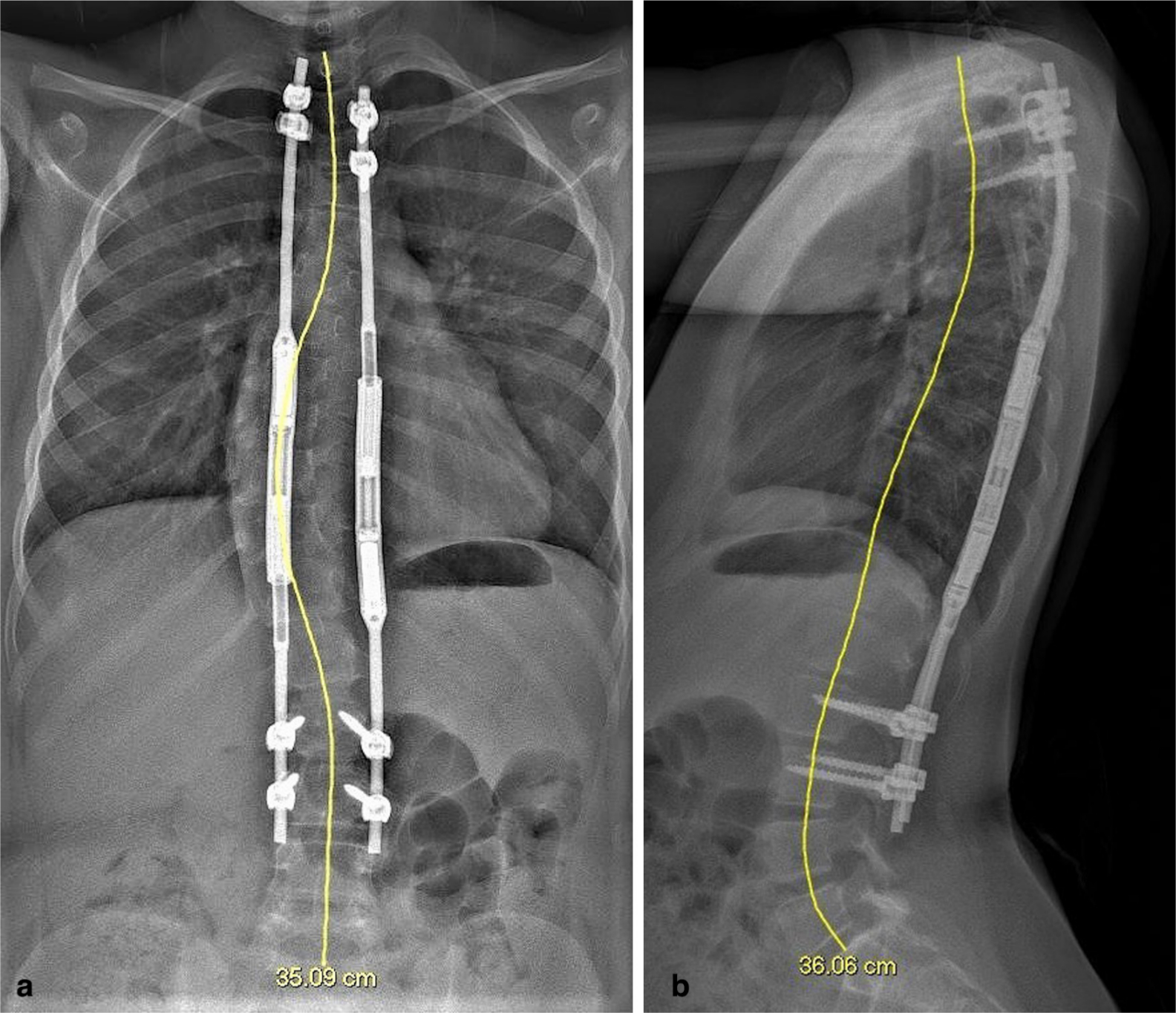
Fig. 2
a) Postoperative coronal view radiograph with T1-S1 measurement. b) Postoperative sagittal view radiograph with T1-S1 measurement.
Subgroup analysis
We identified different subgroups of patients; and separate subgroup analysis was performed on each group. The cohort of patients who developed complications was scrutinised. Various parameters were examined to determine if they were associated with increased risk of having a complication (age, sex, diagnosis, rod configuration, and previous surgery). The cohort of graduates was assessed to determine spine flexibility at the time of fusion. Single versus dual rod cohorts and cohorts of different aetiological diagnoses were also examined to assess the effect of these characteristics on the amount of deformity correction and spinal growth achieved.
Statistical analysis
Descriptive data analysis was performed on Excel 2010 (Microsoft, Redmond, Washington, USA). Equal versus unequal variance was determined via F-test; and accordingly the appropriate Student two-sample t-test was used to compare means. One-way analysis of variance (ANOVA) was used to examine the radiological parameters in different aetiological types of EOS. Chi-squared test was used to compare the cohorts with and without a complication. A p-value of < 0.05 was determined to be statistically significant.
Results
Means of all radiological parameters have significantly improved over the course of treatment. Mean Cobb angle improved by 50% from 70° (53 to 103) pre-operatively to 35° (15 to 71) immediately postoperatively (p < 0.001). This has regressed slightly to 39° (15 to 65) at last follow-up (p < 0.001). This represents a final deformity correction of 45% of the preoperative values. Spinal height parameters (T1-T12 and T1-S1) also showed significant growth. T1-T12 height increased from 198 mm (133 to 26) pre-operatively to 225 mm (157 to 305) at final follow-up; a mean increase of 6.8 mm/year (p < 0.001). Similarly, T1-S1 height has also increased by a mean of 11.25 mm/year from a preoperative value of 316 mm (230 to 425) to 361 mm (271 to 476) at final follow-up (p < 0.001). This is summarized in Table II.
Table II.
Summary of radiological measures.
| Parameter (n) | Mean (range) | Improvement | p-value |
|---|---|---|---|
| Cobb Angle | |||
| Pre-operative (44) | 71° | N\A | |
| Postoperative (44) | 35° | 36° (50%)* | < 0.001 |
| Last FU pre-fusion (44) | 39° | 32° (45%)* | < 0.001 |
| T1-T12 | |||
| Pre-operative (44) | 198 mm | N/A | |
| Last FU (43) | 225 mm | 27 mm (6.8 mm/yr) | < 0.001 |
| T1-T12 | |||
| Pre-operative (44) | 316 mm | N/A | |
| Last FU (43) | 361 | 45 mm (11.3 mm/yr) | < 0.001 |
-
*
in relation to pre-operative values. Student two-sample t-test
-
FU, Follow up
Comparison of radiological parameters of single rods versus dual rods demonstrated that the only significant difference was in the immediate postoperative Cobb angle correction. Dual rods resulted in more correction (54% vs 36%; p < 0.001). There was no difference between the two groups with relation to preoperative Cobb angle (p = 0.081), Cobb angle at last follow-up (p = 0.079), preoperative T1-T12 (p = 0.358), T1-T12 at last follow-up (p = 0.477), preoperative T1-S1 (p = 0.789) or T1-S1 at last follow-up (p = 0.419). All pre-operative and postoperative radiological measures of children with different aetiologies did not show any statistically significant difference on one-way ANOVA analysis (Figure 3).
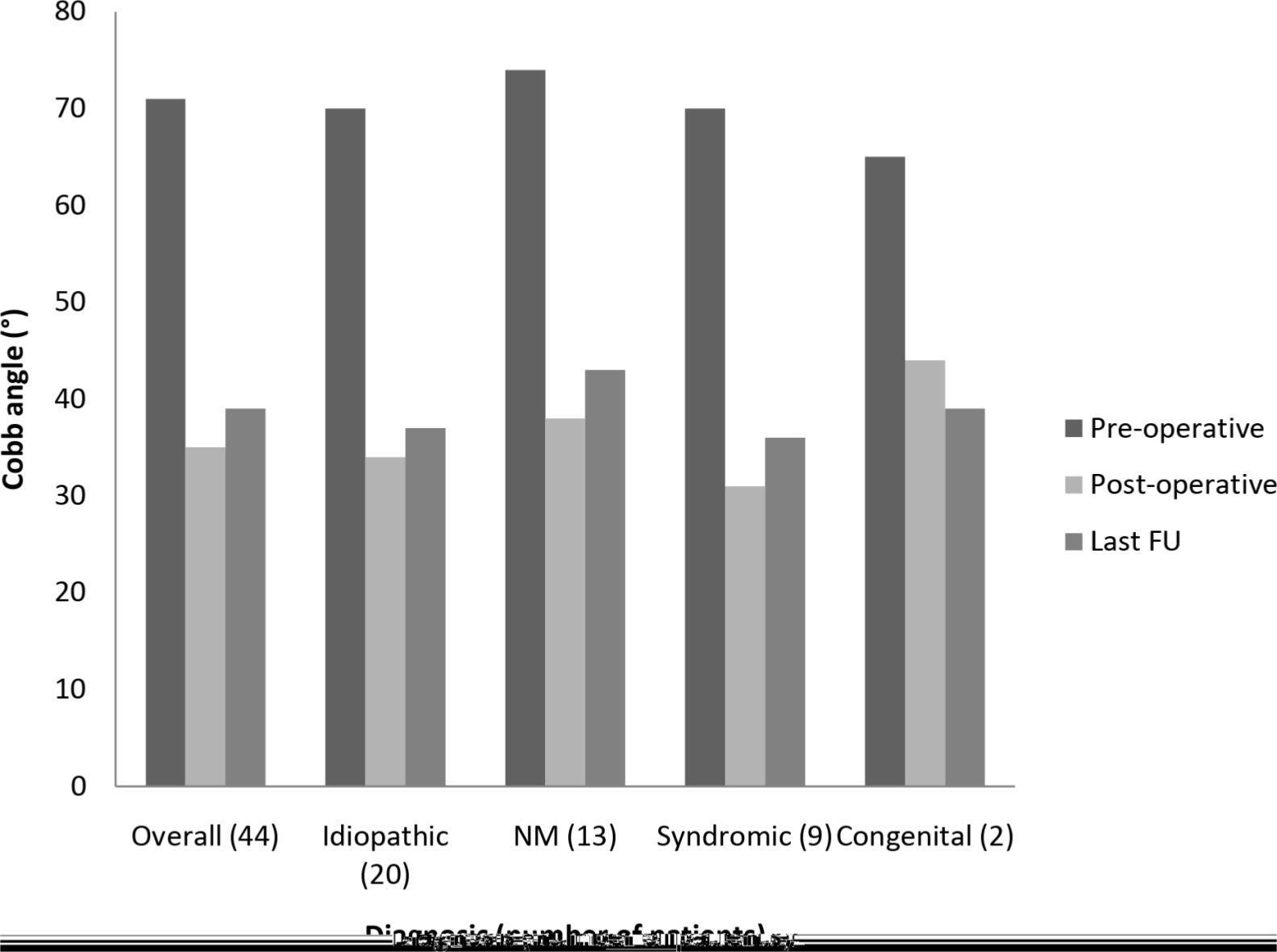
Fig. 3
Comparison of deformity correction in different aetiologies as measured by Cobb angle.
Nine patients have graduated from the MAGEC rod treatment to definitive fusion (and four more patients are currently on the list) at an average of 3.3 years (2 to 5.4) following index procedure. Cobb angle improved from 53° (38 to 65) pre-fusion to 39° (18 to 51) post-fusion. This statistically significant difference (p = 0.04) indicates that the spine retained some flexibility at the end of the MAGEC rod treatment (Figure 4). Proximal and distal fusion levels were all the same levels used for the foundations of the MCGRs with no additional levels needed to be included in the fusion.
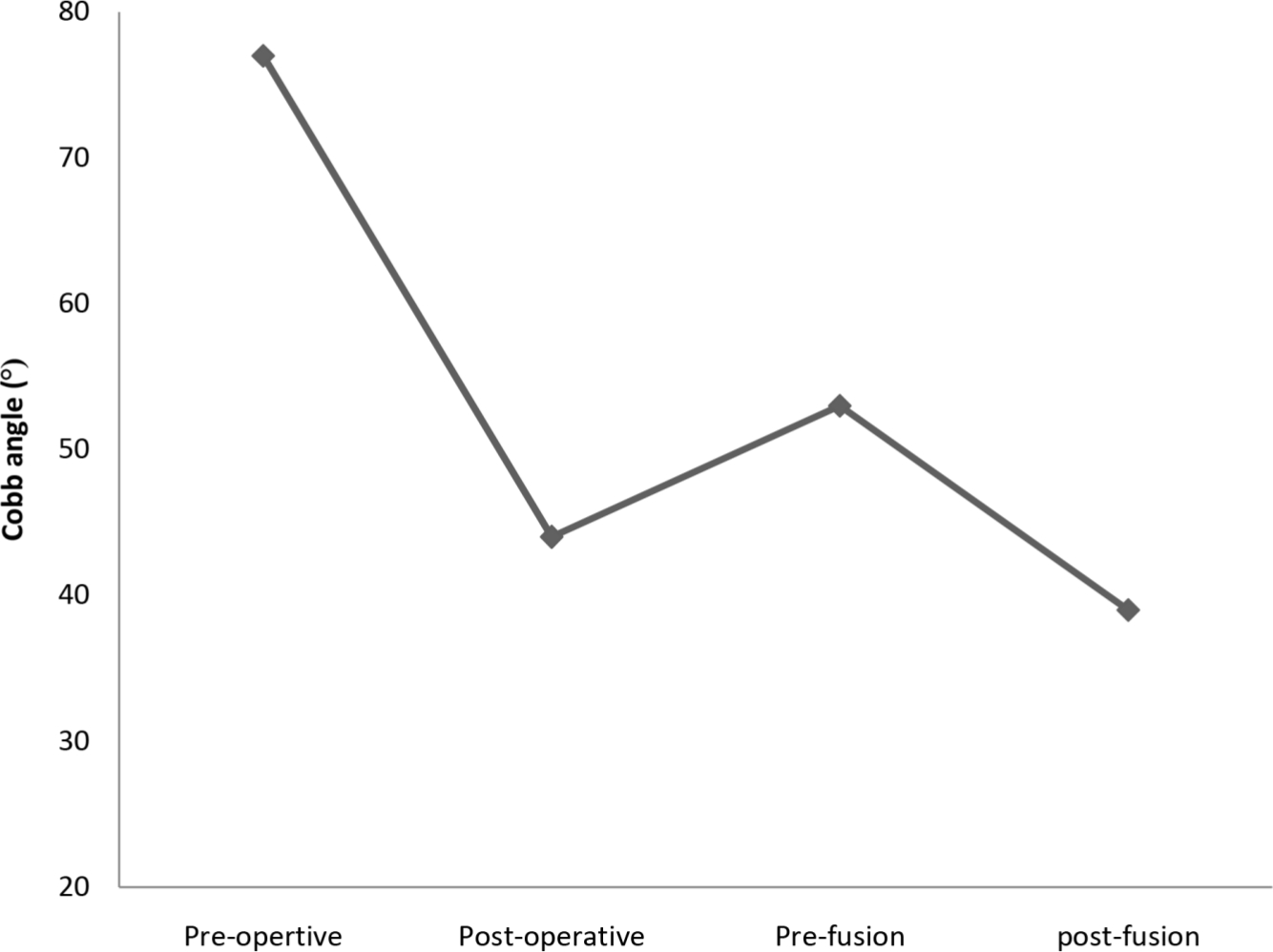
Fig. 4
Comparison of Cobb angles at different time points for the definitive fusion cohort.
A total of 18 clinical complications occurred in ten patients (23%) during their course of follow-up (Table III). These children required 21 unplanned operations between them. Average time for developing a complication was 21.2 months (5 to 36) postoperatively. Three children developed clinically-relevant MCGR-specific complications. These were rod motor failure (n = 2) and jamming of the extensor mechanism (n = 1). Other clinical complications were proximal foundation dislodgement (n = 4), rod fracture (n = 4), prominence of metal (n = 3), distal decompensation (n = 1), infection (n = 2), and proximal junctional kyphosis (n = 1).
Table III.
Summary of postoperative complications.
| Pt | Complication | Time post-surgery (months) | Management | |
|---|---|---|---|---|
| No. | Complication | |||
| 1 | Rod motor failure* | 12 post revision | Definitive fusion | |
| 2 | first second |
Jamming of extensor mechanism* Proximal foundation dislodgement |
26 post index 26 post revision |
Revised to single MAGEC Revision to TGR |
| 3 | first second third |
Proximal foundation dislodgement Proximal foundation dislodgement Proximal foundation prominence |
14 post index 14 post revision 36 post revision |
Revision Revision Removal of one rod |
| 4 | first second |
Proximal foundation dislodgement Deep infection |
5 post index 14 post revision |
Revision to dual MAGEC 2-stage revision to TGR |
| 5 | Distal decompensation | 12 post index | Revision to lower level | |
| 6 | first second |
Rod fracture PJK |
12 post index 33 post revision |
Revision to dual MAGEC 3 revisions |
| 7 | Rod fracture | 27 post index | Revision to dual MAGEC | |
| 8 | first second |
Rod fracture Rod fracture |
12 post index 16 post revision |
Revised to single MAGEC Definitive fusion |
| 9 | first second |
Superficial wound infection Proximal foundation prominence |
N/A 21 post index |
Antibiotics Removal of metal |
| 10 | first second |
Proximal foundation prominence Right Rod motor failure* |
35 post index 36 post index |
Removal of left rod and 2 revisions of proximal foundation Revision to dual MAGEC |
-
TGR, traditional growing rods.
-
*
MAGEC-specific complication (n = 3).
There were four fatigue fractures of rods, three of which occurred in single rod constructs; two in the same patient whose single rod was initially revised with a second single rod. This translates to a 33.3% breakage rate across all patients with a single rod construct. Overall our breakage rate is 6.8% for all patients with MCGR systems.
Two children developed an infection. One deep infection requiring two-stage revision to traditional rods occurred in a child with severe eczema. Staphylococcus aureus was confirmed to be the pathogen responsible on microbiology testing. Another child developed superficial infection within the first month postoperatively. This was treated with oral antibiotics with complete resolution. Both cases had a previous revision surgery prior to developing the infection.
Overall, a total of 34 further revision surgical procedures were performed in 21 patients (47%). During these revision procedures, tissue staining with metal debris was noticed in eight patients. Rods explanted for whatever reason were assessed by the operating surgeon after surgery. We found that 10 MCGR-specific incidents were identified. These included actuator pin breakage (n = 3), rod motor failure (n = 3) and jamming of the rods (n = 4). Only three of these incidents were clinically-relevant and hence were the reason for the revision surgery (two motor failures and one rod jamming). The remaining seven (including all the actuator pin breakages) were discovered incidentally at the time of surgery for MCGR revision having reached its maximum distraction. All explanted implants were sent for mechanical testing and we are currently collating the data from this retrieval analysis.
A separate analysis was made to compare demographic parameters of children who developed a complication versus those without a complication (Table IV). Age, sex, aetiological diagnosis, preoperative Cobb angle, rod configuration and previous surgery were examined independently. Children who developed a complication were younger (7.4 years vs 8 years) and had a higher preoperative Cobb angle (78° vs 68°) than those without a complication. However, neither age nor preoperative Cobb angle was statistically significant with a p-value of 0.46 and 0.054 respectively. Single rod use (p = 0.0001) and previous surgery (p = 0.001) were significantly associated with developing a complication. Sex and aetiological diagnosis did not show significant difference (p = 0.62 and 0.17 respectively).
Table IV.
Comparison of demographics of children with and without complications.
| Complication | No complication | p-value* | |
|---|---|---|---|
| Total number (%) | 10 (23) | 34 (77) | |
|
Sex, n
Male Female |
5 5 |
14 20 |
0.62 |
| Age, mean (range) | 7.4 (5 to 11.6) | 8 (3.7 to 13.6) | 0.46 |
|
Rods, n
Dual Single |
5 5 |
33 1 |
0.0001† |
|
Aetiology, n
Idiopathic NM Syndromic Congenital |
4 1 4 1 |
16 12 5 1 |
0.17 |
|
Pre-operative Cobb angle
Mean (range) |
78 (57 to 103) | 68 (30 to 97) | 0.054 |
|
Previous surgery, n
Previous revision No previous revision |
8 2 |
8 26 |
0.001† |
-
*
Paired t-test was used for comparing means. Chi squared test was used or comparing sex, rod configuration, aetiology, and risk of having a complication with previous revision surgery.
-
†
Statistically significant (p < 0.05).
Discussion
Growing rods remain the gold-standard surgical option in the management of early-onset scoliosis (EOS).1 Recurrent operations to facilitate the lengthening of these constructs carry several problems in terms of anaesthetic risks, higher infection risk and psycho-social issues for the children and their families.10 The emergence of magnetic-controlled growing rod (MCGR) systems offered a potential of reducing these problems considerably. Several authors have reported their results of the use of MCGR systems in the management of EOS. A systematic review on MCGR in 2018, confirmed the efficacy of these systems in maintaining the deformity correction and preserving the spinal growth while keeping an acceptable complication profile.12
To our knowledge, our study represents one of the biggest complete data set in the literature with the longest mean and minimum follow-up periods from a single centre. We report on 44 patients for an average follow-up of 4.1 years with a minimum follow-up of two years. We do not have any patients who were lost to follow-up. Choi et al16 reported on 54 participants in a multicentre study for a mean follow-up of 19.4 months; while Subramanian et al13 reported the longest published mean follow-up of 47 months on 31 patients. The mean age of our cohort of patients (7.9 years) is comparable to other series published.
We report a correction of Cobb angle immediately after the index procedure of 50%. This was maintained at the level of 45% at the final follow-up at an average of 4.1 years. It is worth noting that 41 out of 44 of our cases were primary cases, indicating higher degree of flexibility. This pattern and scale of correction is consistent with other reports of similar cohorts. After initial surgery, Ridderbusch et al17 reported 54% correction in 24 primary cases; Keskinen et al18 reported 46% correction in 23 primary cases; while Subramanian et al13 reported 36% correction in 16 primary cases.
Similarly, in our study we noted significant spine growth of both T1-T12 and T1-S1 heights, mirroring that of other reports.12,13 However, to our knowledge, our length measurement technique is novel. We used the unique measurement ability of our PACS system (Carestream Health, Rochester, New York, USA) to measure the length of the curved line representing the actual deformity on both coronal and sagittal views, taking the mean of both measurements after calibration (Figure 1-2). Previous reports in the literature measured the perpendicular height of T1-T12 and T1-S1. While this represents a reasonably accurate proxy for spinal growth of the normal straight spine, perpendicular height should not be considered a true representative of the growth of a curved spine.
We examined the effect of sex, age, aetiological diagnosis, and number of rods on the improvement of radiological parameters at different time points. The only significant difference was noticed in the Cobb angle after the index operation favouring the dual rods as compared to single constructs (55% vs 36%; p < 0.001). However, this difference was neither as profound nor significant at last follow-up (46% vs 42%; p 0.079). This is also consistent with other reports in the literature.13
One of the questions that remained largely unanswered in the literature is whether the spine remains flexible at the end of the MCGR treatment. If so, this would allow further correction of the deformity at the time of definitive fusion. This has been investigated previously mainly for the traditional growing rods. Flynn et al,19 in his review of 62 patients who progressed from TGR to fusion at an average of ive years, reported that > 60% of the patients in their series developed spontaneous fusion; with 24% requiring spinal osteotomies. This is similar to the earlier results of Cahill et al,20 who also reported a high rate (89%) of spontaneous fusion at the end of the TGR treatment of nine children followed-up for 9.6 years. This is expected following TGR treatment with multiple open lengthening surgical procedures. As for MCGR, in his review of five MCGR graduates, Cheung et al21 did not find any further improvement post-fusion at a mean of 6.5 years after initial implantation. However, we had a contrasting experience with our cohort of nine patients who graduated from MCGR to definitive fusion. The spine remained largely flexible, allowing an average of additional correction of 26% post-fusion in five patients (56%); with two patients achieving correction of more than 50%. Three patients required only limited osteotomies (two to three-level facetectomy) at the fusion surgery.
In our series, ten children (23%) developed complications. This is lower than most other reports of similar cohorts in the literature.13,22 Our overall complication rate per patient was also lower at 0.4 per patient, compared to Subramanian et al13 at 0.74 per patient. When this was adjusted for the length of follow-up, our complication rate was 0.1 per patient per year, the lowest in the literature.12 We report three MCGR-specific complications in three patients (6%), with a rate of 0.06 MGCR-specific complications per patient and 0.02 per patient per year. However, we identified a number of MCGR-related issues that were not clinically relevant and were only noticed incidentally at the time of revision of the rods that reached their maximum distraction capacity. Two broken actuator pins, two mechanical rod failures and one rod jamming were noticed in explanted rods from five asymptomatic patients. All these patients have reached the end of their rod treatment satisfactorily and with no clinical or radiological concerns. If we include all these incidents as complications, our adjusted overall complication rates become 34%, 0.52 per patient and 0.13 per patient per year. MCGR-specific complications similarly would increase to 18%, 0.22 per patient and 0.06 per patient per year. However, we believe that these adjusted rates are not a true reflection of the clinical situation.
Two children developed an infection (4%) during their course of treatment. Choi et al16 reported 3.7% rate of infection in his series of 54 patients with mean follow-up of 19.4 months, while Lebon et al23 and Subramanian et al13 reported infection rates of 7% and 16% respectively. Both cases in our series had a revision surgery prior to developing the infection. This is in agreement with previous studies reporting higher infection rate in revision cases of growing rods.24
In our study, we investigated various patient parameters in relation to the risk of developing a complication. Five of the six children who had single constructs in our series developed a complication. This is widely supported in the literature by other studies on MCGR systems;13,14 as well as larger earlier studies on growing rods, even though not specifically MCGRs.10 A recent systematic review of MCGR complications by Thakar et al12 recommends against the use of single rods. Our results support this recommendation. Similarly, eight of our ten children with a complication had a revision surgery prior to developing a complication. Bess et al10 reviewed 140 patients treated with growing rods and reported a 24% increased risk of developing a complication with each additional procedure beyond the index surgery.
Other reports on growing rods (MCGRs and TGRs) suggested that children who developed a complication were younger than those who did not.10,13 While our data suggests a similar trend, the age difference between the two groups in our series (complication and no complication) was not significant. Similarly, sex, initial Cobb angle, and aetiological diagnosis were not found to be significantly different between the two groups in our series.
We report an overall revision rate of 47% in our series. Furthermore, we currently have five more children on the list for revision surgery. These children have not had any previous revision surgery since their index procedure, indicating that our revision rate will increase once these planned procedures are performed. This rate is lower than that reported by Subramanian et al13 (64%); yet higher than Lebon et al23 (30%). However, two points are worth noting. Firstly, we have significantly longer follow-up of 4.1 years compared to 18.4 months by Lebon et al. Secondly, 11 out of the 21 patients who had revision in our series had it for having reached the rods’ utmost distraction magnitude; an anticipated and awaited outcome of treatment. This is in contrast with other reports, in which the main indication for revision surgery was to treat a complication. In our series, 23% of our patients had unplanned surgery at 4.1 years of follow-up; well below the average of 33% reported in the literature at 2.5 years in a systematic review published in 2018.12
More recently, concerns have risen regarding various aspects of MCGR systems.25 Their ability to maintain their distraction ability over time, their effect on the adjacent soft tissues with metal debris deposition, implant failures and serum metal ion concentration are among these concerns. Researchers have taken the quest to investigate these concerns.
Sankar et al26 described the law of diminishing returns of distractions upon repeated lengthening of TGRs. He attributed this to the increasing spinal stiffness over time. By avoiding repeated open lengthening procedures, MCGRs were hoped to avoid this phenomenon. However, Ahmad et al27 demonstrated a near linear decline in the distraction of MCGRs in 35 patients over a 30 month period of follow-up, indicating that the law of diminishing returns also applies to MCGRs. However, the pattern of this decline is gradual; in contrast to the rapid initial decline described in TGRs. Despite that, our data suggest a significant increase in overall spine length and deformity correction over the treatment period.
We found that eight children had metal debris staining of the soft tissues at revision surgery. Four of these rods were working well at extraction and four were not distracting (two broken actuator pins, one jammed, and one motor failure). Teoh et al28 reported similar findings in four out of five patients who had revision of MCGRs. Subsequently several authors investigated the association between the implant mechanism of failure and metallosis.29-31 Fractured pins, surface abrasive damage, non-functional radial bearing and off-axis loading were found to be mechanisms for generating titanium debris. Whether this is also associated with increased serum levels of metal ions, and the long-term effects of this remain unclear.25 There is ongoing work investigating all aspects of implant failures.
A limitation of our study is the inherent nature of the retrospective design. However, due to the nature of the condition, the majority of the literature adopts a similar design. Another limitation is the lack of reporting on the effect of MCGRs on sagittal balance. However, the effect of a posteriorly based distraction system on the sagittal profile of the growing spine is understood and predicted. Finally, we accept the heterogeneity of the aetiologies in our cohort. This is also reflected in the majority of the published literature. However, dissecting this further is the aim of another ongoing study in our centre. Our study has multiple strengths. We present one of the largest series with the longest follow-up (minimum and mean), with a glimpse on the end of the treatment journey and analysis of complication profile.
In summary, this study demonstrates that MCGR remain an effective tool in the management of EOS; with a significant ability to correct the deformity and support the spine growth. We recommend against the use of single MCGRs constructs. In our series, MCGRs has a complication profile and revision rate lower than the average published in literature. We found that having a revision surgery increases the likelihood of subsequently developing a complication. We also demonstrated that the spine retained high degree of flexibility at the end of treatment; allowing further correction at the time of definitive fusion. Further work is required to investigate various failure mechanisms.
References
1. Abdelaal A , Nnadi C . Is There a Gold-Standard Surgical Option? In: Nnadi C, editor. Early Onset Scoliosis: A Comprehensive Guide from the Oxford Meetings . Stuttgart : Thieme , 2016 : 255 – 262 . Google Scholar
2. Akbarnia BA . Management themes in early onset scoliosis . J Bone Joint Surg Am . 2007 ; 89 ( Suppl 1 ): 42 – 54 . Crossref PubMed Google Scholar
3. Harrington PR . Treatment of scoliosis. correction and internal fixation by spine instrumentation . J Bone Joint Surg Am . 1962 ; 44-A : 591 – 610 . PubMed Google Scholar
4. Moe JH , Kharrat K , Winter RB , Cummine JL . Harrington instrumentation without fusion plus external orthotic support for the treatment of difficult curvature problems in young children . Clin Orthop Relat Res . 1984 ; 185 : 35 – 45 . PubMed Google Scholar
5. Klemme WR , Denis F , Winter RB , Lonstein JW , Koop SE . Spinal instrumentation without fusion for progressive scoliosis in young children . J Pediatr Orthop . 1997 ; 17 ( 6 ): 734 – 742 . PubMed Google Scholar
6. Blakemore LC , Scoles PV , Poe-Kochert C , Thompson GH . Submuscular Isola rod with or without limited apical fusion in the management of severe spinal deformities in young children: preliminary report . Spine (Phila Pa 1976) . 2001 ; 26 ( 18 ): 2044 – 2048 . Crossref PubMed Google Scholar
7. Mineiro J , Weinstein SL . Subcutaneous rodding for progressive spinal curvatures: early results . J Pediatr Orthop . 2002 ; 22 ( 3 ): 290 – 295 . PubMed Google Scholar
8. Akbarnia BA , Marks DS , Boachie-Adjei O , Thompson AG , Asher MA . Dual growing rod technique for the treatment of progressive early-onset scoliosis: a multicenter study . Spine (Phila Pa 1976) . 2005 ; 30 ( 17 Suppl ): S46 – S57 . Crossref PubMed Google Scholar
9. Akbarnia BA , Breakwell LM , Marks DS , et al. Dual growing rod technique followed for three to eleven years until final fusion: the effect of frequency of lengthening . Spine (Phila Pa 1976) . 2008 ; 33 ( 9 ): 984 – 990 . Crossref PubMed Google Scholar
10. Bess S , Akbarnia BA , Thompson GH , et al. Complications of growing-rod treatment for early-onset scoliosis: analysis of one hundred and forty patients . J Bone Joint Surg Am . 2010 ; 92 ( 15 ): 2533 – 2543 . Crossref PubMed Google Scholar
11. Cheung KM , Cheung JP , Samartzis D , et al. Magnetically controlled growing rods for severe spinal curvature in young children: a prospective case series . Lancet . 2012 ; 379 ( 9830 ): 1967 – 1974 . Crossref PubMed Google Scholar
12. Thakar C , Kieser DC , Mardare M , et al. Systematic review of the complications associated with magnetically controlled growing rods for the treatment of early onset scoliosis . Eur Spine J . 2018 ; 27 ( 9 ): 2062 – 2071 . Crossref PubMed Google Scholar
13. Subramanian T , Ahmad A , Mardare DM , et al. A six-year observational study of 31 children with early-onset scoliosis treated using magnetically controlled growing rods with a minimum follow-up of two years . Bone Joint J . 2018 ; 100-B ( 9 ): 1187 – 1200 . Crossref PubMed Google Scholar
14. Thompson W , Thakar C , Rolton DJ , Wilson-MacDonald J , Nnadi C . The use of magnetically-controlled growing rods to treat children with early-onset scoliosis: early radiological results in 19 children . Bone Joint J . 2016 ; 98-B ( 9 ): 1240 – 1247 . Crossref PubMed Google Scholar
15. Munigangaiah S , Brown P , Mohamed M , et al. A novel technique for the subfascial insertion of magnetically controlled growing rods - The Alder Hey technique . J Craniovertebr Junction Spine . 2018 ; 9 ( 4 ): 250 – 253 . Crossref PubMed Google Scholar
16. Choi E , Yaszay B , Mundis G , et al. Implant Complications After Magnetically Controlled Growing Rods for Early Onset Scoliosis: A Multicenter Retrospective Review . J Pediatr Orthop . 2017 ; 37 ( 8 ): e588 – e92 . Crossref PubMed Google Scholar
17. Ridderbusch K , Rupprecht M , Kunkel P , Hagemann C , Stücker R . Preliminary Results of Magnetically Controlled Growing Rods for Early Onset Scoliosis . J Pediatr Orthop . 2017 ; 37 ( 8 ): e575 – e580 . Crossref PubMed Google Scholar
18. Keskinen H , Helenius I , Nnadi C , et al. Preliminary comparison of primary and conversion surgery with magnetically controlled growing rods in children with early onset scoliosis . Eur Spine J . 2016 ; 25 ( 10 ): 3294 – 3300 . Crossref PubMed Google Scholar
19. Flynn JM , Tomlinson LA , Pawelek J , et al. Growing-rod graduates: lessons learned from ninety-nine patients who completed lengthening . J Bone Joint Surg Am . 2013 ; 95 ( 19 ): 1745 – 1750 . Crossref PubMed Google Scholar
20. Cahill PJ , Marvil S , Cuddihy L , et al. Autofusion in the immature spine treated with growing rods . Spine (Phila Pa 1976) . 2010 ; 35 ( 22 ): E1199 – E1203 . Crossref PubMed Google Scholar
21. Cheung JPY , Yiu K , Kwan K , Cheung KMC . Mean 6-Year Follow-up of Magnetically Controlled Growing Rod Patients With Early Onset Scoliosis: A Glimpse of What Happens to Graduates . Neurosurgery . 2019 ; 84 ( 5 ): 1112 – 1123 . Crossref PubMed Google Scholar
22. Studer D , Heidt C , Büchler P , Hasler CC . Treatment of early onset spinal deformities with magnetically controlled growing rods: a single centre experience of 30 cases . J Child Orthop . 2019 ; 13 ( 2 ): 196 – 205 . Crossref PubMed Google Scholar
23. Lebon J , Batailler C , Wargny M , et al. Magnetically controlled growing rod in early onset scoliosis: a 30-case multicenter study . Eur Spine J . 2017 ; 26 ( 6 ): 1567 – 1576 . Crossref PubMed Google Scholar
24. Kabirian N , Akbarnia BA , Pawelek JB , et al. Deep Surgical Site Infection Following 2344 Growing-Rod Procedures for Early-Onset Scoliosis: Risk Factors and Clinical Consequences . J Bone Joint Surg Am . 2014 ; 96 ( 15 ): e128 . Crossref PubMed Google Scholar
25. Tsirikos AI , Roberts SB . Magnetic Controlled Growth Rods in the Treatment of Scoliosis: Safety, Efficacy and Patient Selection . Med Devices (Auckl) . 2020 ; 13 : 75 – 85 . Crossref PubMed Google Scholar
26. Sankar WN , Skaggs DL , Yazici M , et al. Lengthening of dual growing rods and the law of diminishing returns . Spine (Phila Pa 1976) . 2011 ; 36 ( 10 ): 806 – 809 . Crossref PubMed Google Scholar
27. Ahmad A , Subramanian T , Panteliadis P , et al. Quantifying the 'law of diminishing returns' in magnetically controlled growing rods . Bone Joint J . 2017 ; 99-B ( 12 ): 1658 – 1664 . Crossref PubMed Google Scholar
28. Teoh KH , Winson DM , James SH , et al. Magnetic controlled growing rods for early-onset scoliosis: a 4-year follow-up . Spine J . 2016 ; 16 ( 4 Suppl ): S34 – S39 . Crossref PubMed Google Scholar
29. Panagiotopoulou VC , Tucker SK , Whittaker RK , et al. Analysing a mechanism of failure in retrieved magnetically controlled spinal rods . Eur Spine J . 2017 ; 26 ( 6 ): 1699 – 1710 . Crossref PubMed Google Scholar
30. Rushton PRP , Smith SL , Forbes L , et al. Force Testing of Explanted Magnetically Controlled Growing Rods . Spine (Phila Pa 1976) . 2019 ; 44 ( 4 ): 233 – 239 . Crossref PubMed Google Scholar
31. Rushton PRP , Smith SL , Kandemir G , et al. Spinal Lengthening With Magnetically Controlled Growing Rods: Data From the Largest Series of Explanted Devices . Spine (Phila Pa 1976) . 2020 ; 45 ( 3 ): 170 – 176 . Crossref PubMed Google Scholar
Author contributions
A. Abdelaal: Main author, Collected and analyzed the data, Wrote the manuscript.
S. Munigangaiah: Reviewed and edited the manuscript.
J. Trivedi: Reviewed and edited the manuscript.
N. Davidson: Reviewed and edited the manuscript.
Funding statement
No benefits in any form have been received or will be received from a commercial party related directly or indirectly to the subject of this article.
© 2020 Author(s) et al. This is an open-access article distributed under the terms of the Creative Commons Attributions licence (CC-BY-NC-ND), which permits unrestricted use, distribution, and reproduction in any medium, but not for commercial gain, provided the original author and source are credited.
