





Abstract
Neurogenic heterotopic ossification (NHO) is a disorder of aberrant bone formation affecting one in five patients sustaining a spinal cord injury or traumatic brain injury. Ectopic bone forms around joints in characteristic patterns, causing pain and limiting movement especially around the hip and elbow. Clinical sequelae of neurogenic heterotopic ossification include urinary tract infection, pressure injuries, pneumonia and poor hygiene, making early diagnosis and treatment clinically compelling. However, diagnosis remains difficult with more investigation needed. Our pathophysiological understanding stems from mechanisms of basic bone formation enhanced by evidence of systemic influences from circulating humor factors and perhaps neurological ones. This increasing understanding guides our implementation of current prophylaxis and treatment including the use of non-steroidal anti-inflammatory drugs, bisphosphonates, radiation therapy and surgery and, importantly, should direct future, more effective ones.
Introduction
Heterotopic ossification (HO) is a process of benign bone formation and growth outside of normal skeletal locations. It is associated with numerous local and systemic conditions. These include hip replacement and acetabular surgery, soft-tissue and bony trauma, burns, rare congenital diseases such as fibrodysplasia ossificans progressiva, rheumatologic diseases such as ankylosing spondylitis, and neurological conditions including tumours of the central nervous system, encephalitis, traumatic brain injury and spinal cord injury.1-4
Neurogenic heterotopic ossification (NHO) is a devastating complication of major central nervous system trauma seen in more than 20% of patients with traumatic brain injury and/or spinal cord injury,1 appearing in characteristic patterns around major joints. Significant morbidity can be observed at the site of this formation of new bone, including pain and loss of motion especially around joints. In addition, the development of NHO increases the risk of complications such as urinary tract infection (UTI) and pressure ulcers, which can significantly impair quality of life.2 The aetiology is not clearly known; however, there is some evidence of a complex interplay between local and systemic factors including neuroendocrine, genetic and extrinsic factors. Mainstays of management include primary and secondary prevention with radiation and non-steroidal anti-inflammatory drugs (NSAIDs). Traditionally, once matured, surgical excision of HO may be indicated. Success and recurrence appear to be strongly correlated to the degree of CNS injury.2,4,5 NHO poses a multitude of challenges to the neurologically injured patient. This review describes the anatomy, diagnosis, prevention, and management of neurogenic heterotopic ossification related to traumatic brain and spinal cord injury.
Search strategy and selection criteria
We searched the PubMed Database, the Cochrane Library, and Google Scholar for references to include in this review. Publications were primarily chosen if published after 2005, however, there is a significant amount of historically important literature from before 2005 that we deemed appropriate for inclusion. Additionally, much of the seminal work on pharmacological prevention and epidemiology is over a decade old. These references were included as they provide valuable information that is the most recent. We used the search terms “neurogenic heterotopic ossification”, “heterotopic ossification and spinal cord injury”, “heterotopic ossification and traumatic brain injury”, “heterotopic ossification prevention” and “bisphosphonates”. Several review articles that provide detailed descriptions of neuroendocrine interactions and population based epidemiologic data were included. Our search was not limited to the English language. We excluded publications that we deemed redundant and/or not specific to neurogenic causes of heterotopic ossification.
Epidemiology
Neurogenic heterotopic ossification (NHO) is well-described in the literature and can be generally divided into two categories: 1) disease related to traumatic brain injury (TBI-HO); and 2) disease related to spinal cord injury (SCI-HO). Gender dependence varies widely in the literature, ranging from little to no relationship,3 to a prevalence approximately 2.5 times greater in males,1,2,5 to a prevalence three times higher in females.4 A correlation with age is suggested, with NHO being more common in patients between 20 and 30 years old, although this may be related to the age range at which TBI and SCI are most frequent.2,6,7 Larson et al8 have suggested a relationship between human leukocyte antigen (HLA) B27 and the development of SCI-HO, whereas others, such as Garland et al,9 have not been able to show any such correlation. At this time there appears to be no consensus as to whether there is a clear genetic predisposition to developing sporadic post-traumatic NHO.1,3,5
Prevalence and patterns of ossification
Traumatic brain injury
Between 8% and 20% of patients with traumatic brain injury go on to develop clinically significant NHO around a joint, as defined by pain and decreased range of movement (ROM) with radiological evidence of abnormal bone formation.1,4,10,11 Both upper and lower extremities are affected, with the most common joint implicated being the hip and thigh, which may be implicated in as high as two-thirds of cases.4,10 In these patients, HO is seen in three characteristic locations; most commonly it occurs inferomedial to the hip and is associated with adductor spasticity. It also occurs anterior to the hip between the anterior superior iliac spine and femur, and finally, posterior to the hip.10 The elbow is the next most common location of TBI-HO. The specific location relative to the elbow depends on the presence of flexor or extensor spasticity, with flexor spasticity resulting in anterior HO and extensor spasticity resulting in posterior HO.10 TBI-HO of the shoulder and knee is less commonly seen, and the wrist, ankle, hands and feet are rarely involved.1 Trauma to the affected joint area appears to guide the severity of the NHO, in addition to the severity of TBI itself.12
Approximately 90% of TBI patients with a fracture or dislocation of the elbow go on to develop HO about the affected elbow, whereas the rate of clinically relevant HO of the elbow following elbow trauma in the non-TBI patient is between 3% and 6%.4,13
Spinal cord injury
Clinically significant HO develops in about 20% of patients with a spinal cord injury.2,3 It always occurs below the neurological level of the injury, and is strongly correlated with the degree of completeness of the spinal cord injury.1-3 Although SCI-induced NHO is seen in association with spasticity, whether HO precedes spasticity or vice versa is unclear. SCI-induced NHO is more commonly seen in cervical and thoracic injuries than lumbar injuries, with between 3% and 8% of these patients developing joint ankylosis.1-3 Even more than in TBI, SCI-HO occurs predominantly in the hip (up to 97% of SCI-HO)10; in this setting, it is not uncommon for ankylosis of the hip joint to occur. Medial disease occurs more often than lateral disease around the hip, with ossified tissues extending from the pubic symphysis to the anteromedial femoral shaft posterior to the femoral neurovascular structures. Ossification is also seen anteriorly involving the iliopsoas and femoral neurovascular structures, laterally within gluteus minimus and posteriorly extending from the ilium to the posterior femur encasing the sciatic nerve. HO of the knee and distal femur are less common locations seen in SCI, and similarly to TBI-HO, the wrists, ankles, hands and feet are almost never involved.13 SCI-HO about the knee may occur anteriorly, medially and posteriorly. Anteriorly ossification occurs beneath the extensor mechanism, medially about the MCL, and posteriorly about the hamstring insertion. Ankylosis is less common in the shoulder.13 Posteriorly, HO forms in the teres muscles, often encasing the axillary nerve and anteriorly HO forms in the anterior capsule. SCI-HO about the elbow develops anteriorly and posteriorly from the humerus to the olecranon, encasing the ulnar nerve and often causing ankylosis.1 Of patients who develop SCI-HO, 55% will have multiple joints involved.2
Similarly to both SCI-HO and TBI-HO, heterotopic ossification related to cardiovascular accident (CVA) most commonly affects the hip joint. There is limited data regarding CVA-HO, although it appears to predominantly affect the hemiparetic side. It is unknown whether CVA-HO is more commonly seen in patients with an ischaemic or haemorrhagic stroke.14
Pathophysiology
The development of heterotopic ossification is related to the interplay between complex local and systemic factors that lead to the increased activity of osteoblasts and the preferential differentiation of pluripotent mesenchymal cells into bone forming osteoblast. It is generally recognised that the signal to begin this process can be traumatic, genetic, or neurogenic. Three conditions are required for the formation of ectopic bone: osteogenic precursors, an inducing agent and a permissive environment.15
Patients with SCI and TBI have an altered serum. Humoral factors play a role as a potential inducing agent of NHO formation or serve to enrich the environment by which the NHO forms.16,17 Many factors such as TGF-β, insulin-like growth factor II, platelet-derived growth factor, interleukin-1, and interleukin-6 are seen in varying levels in experimental rat models18,19 and have been shown to increase activity of osteoblastic cells from animals with SCI.16 Serum analyses of paraplegic patients and neuro-intact patients indicates that there are significantly greater levels of alkaline phosphatase in the paraplegic group.17 Furthermore, patients with long bone fractures in addition to TBI have two-fold faster union rates and up 50% more callus formation.15,20 Serum taken from patients with TBI contains circulating factors that stimulate the preferential differentiation of mesenchymal cells into osteoblast.21
The relationship between the nervous system and bone is not completely understood but what is clear is that specific nervous system neurotransmitters have a direct effect on bone metabolism (Fig. 1). It has been well established that bone is densely innervated.22 Immunohistochemical studies have shown that sympathetic nerve fibres with vasoactive intestinal peptide (VIP) are readily seen in bone.23 This led to the investigation of other neurotransmitter’s and their potential role in the development of increased ectopic bone formation. Glutamate, calcitonin gene-related protein, substance P and catecholamines have all been isolated from bone and shown to upregulate osteoblastic activity and downregulate osteoclastic activity.24 Recent research has shown that leptin, a hormone important in the regulation of energy intake and expenditure, influences bone formation by way of the hypothalamus and sympathetic nervous system.25 Relevant to NHO, leptin has been shown to be elevated in SCI rat fracture models.26
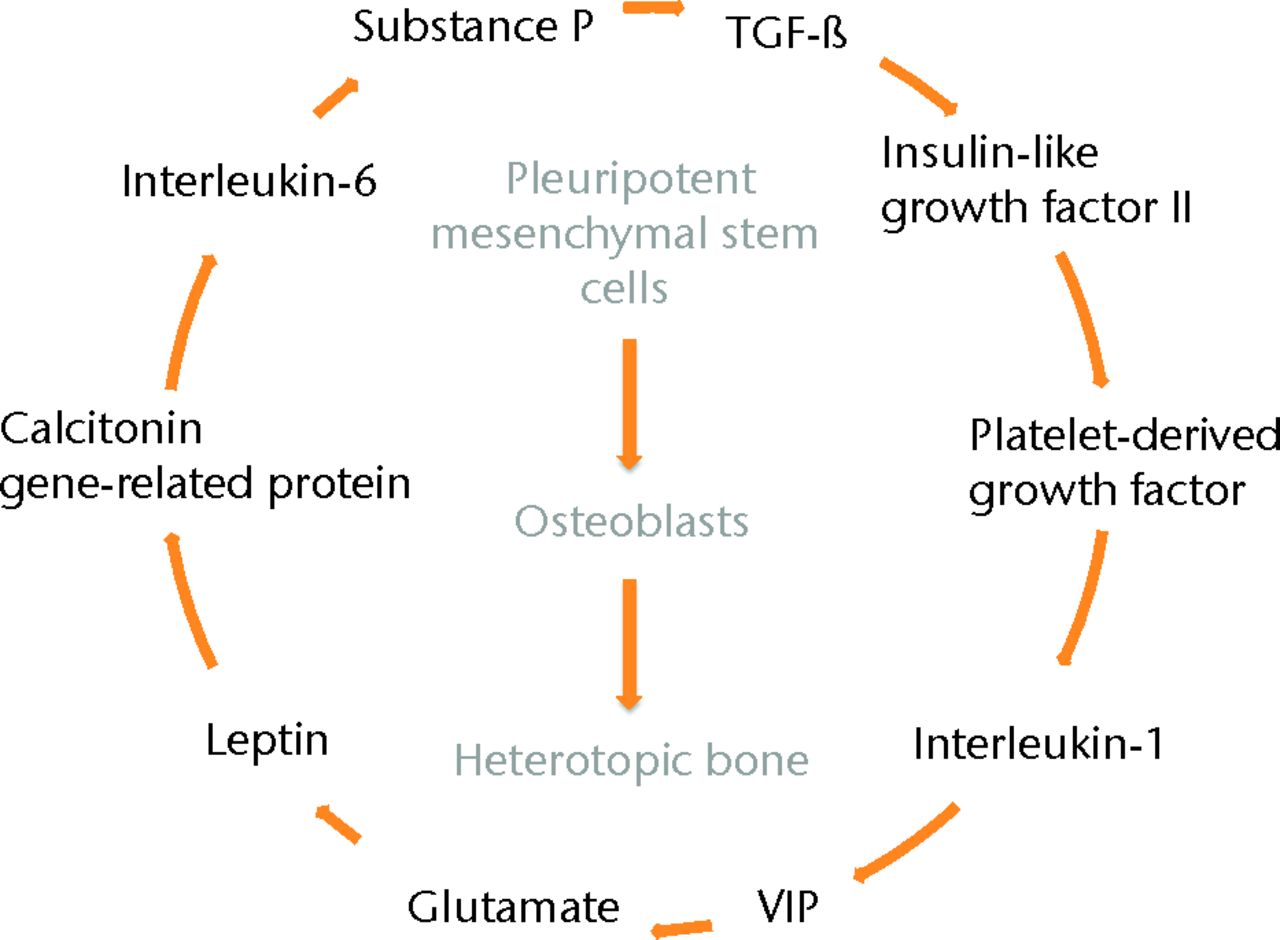
Fig. 1
Diagram depicting the complex and poorly understood interplay between neurohumoral factors and the development of heterotopic bone formation. At the centre is the stimulation of osteoblasts to lay down ectopic bone.
Clinical evaluation and diagnosis
Like normotopic osteogenesis, NHO progresses through predictable stages of maturation. The developmental stage can be helpful in determining when it is most appropriate to initiate therapy. The three stages of HO maturation are based on histological, bone scan and plain films findings.1 The early stage consists of immature bone composed of well-organised collagen matrix and speckled calcification. Collagen bundles are organised along lines of tension. Standard radiology is not sensitive enough to detect early-phase HO, but bone scans and MRI can identify typical findings.19,23,24 The intermediate stage is characterised by intense inflammation, vascularisation and increased calcification. Immature peri-articular ossification can be seen on radiographs. Finally, mature HO is seen histologically as mature bone with radiological findings similar to normal remodeling bone.1
The diagnosis of HO begins with physical examination. Unfortunately, it often presents with a similar picture to septic arthritis and deep vein thrombosis with warmth, erythema, swelling and limited ROM.1,5,24,27 The mean time from injury to diagnosis of HO is two months, but may range from two weeks to one year.1 The formation of HO typically presents clinically before it can be diagnosed radiologically. Traditionally, a 3-phase bone scan has been considered the most sensitive method for early imaging-based detection of HO, with detection as early as two weeks after the onset of symptoms. However, more recent data suggest that MRI shows changes consistent with HO formation one to two days after the onset of symptoms.24 Standard radiological diagnosis of HO generally cannot be made until around three to six weeks after the onset of symptoms. Early MRI findings of HO around the knee include interstitial oedema, thickening of the intramuscular connective tissue, joint effusion, and a lacy muscular pattern seen with STIR sequencing.5,11,24
Evaluation with computed tomography (CT) substantially enhances understanding of the extent of HO and its three-dimensional (3D) relationship with the joint and surrounding neurovascular structures. Therefore, 3D reconstructions can aid in choosing the safest and most affective surgical approach for resection.28 CT with 3D reconstruction can be an integral part of the standard pre-operative assessment in patients undergoing surgical excision of HO (Fig. 2).
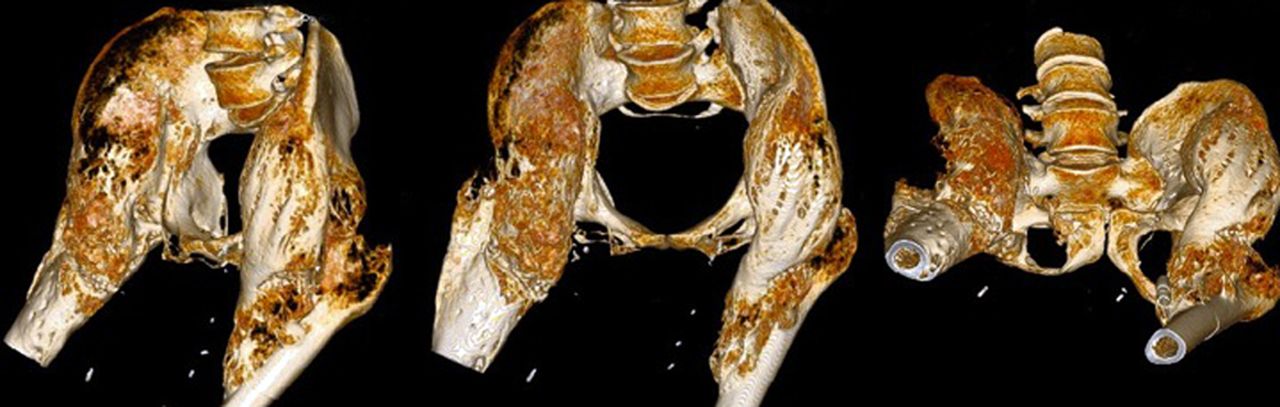
Fig. 2
A 40-year-old male patient sustained an American Spinal Injury Association (ASIA) grade-A spinal cord injury from a gunshot at the level of T10. At five years after injury, three-dimensional CT images show massive bilateral heterotopic ossification (HO) of the hips with joint ankylosis. Complications of the extensive HO include recalcitrant sacral pressure ulcers and an inability to sit in a wheelchair.
Serum alkaline phosphatase levels significantly increase over the first six to 12 weeks after injury in patients who develop HO, and this may be a helpful adjunct in the diagnosis of early HO, especially in patients who cannot report pain or in whom physical exam is not possible or practical.1,2,5 Normalisation of serum alkaline phosphatase levels does not correlate with maturation of HO, nor does the peak alkaline phosphatase level correlate with peak osteogenic activity.3
Management
NSAIDs
Multiple randomised controlled trials support the use of various NSAIDs for primary prevention of NHO following CNS injury.29,30 The mechanism is believed to be through the systemic inhibition of prostaglandins, which in turn regulate mesenchymal cell differentiation into osteoblastic cells that contribute to the new bone.29,30 A significant decline in the development of HO has been shown in a group of patients started on a six-week course of empiric indomethacin (non-selective COX inhibitor) three weeks from the time of CNS injury when compared with a control group.29 In a follow-up trial, similar results were obtained with the use of rofecoxib (selective COX-2 inhibitor).30 In this trial 76 patients were randomised into two groups: a treatment group with 25 mg of rofecoxib daily for four weeks, and a non-treatment control group. After one month, there was a significantly lower rate of HO in the treatment group (13.4%) compared with the placebo group (33%). These data suggest a significant decrease in HO when rofecoxib is used as a primary prevention.30 Rofecoxib was taken off the market by the United States Food and Drug Administration (FDA) in September 2004,31 indomethacin is now the gold standard pharmacological prevention of HO. Optimal time for initiating therapy is within two months of the injury and should be carried out for four to six weeks. Standard dosing is 75 mg long-acting indomethacin daily, or 25 mg standard release indomethacin three times daily.29,30
Bisphosphonates
The role of bisphosphonates on the inhibition of pathological calcification in vivo was originally described in the late 1960s.32 Since that time numerous studies have shown the efficacy of bisphosphonates as primary prevention for NHO in spinal cord and traumatic brain injured patients.33,34 Disodium etidronate was the first bisphosphonate studied in humans and is the most extensively studied bisphosphonate for the prevention and treatment of NHO. Numerous studies have shown etidronate to be useful in primary prevention as well as in reducing NHO in both the early phases of disease and later phases of disease.35-37 There are many proposed mechanisms by which bisphosphonates work; however, it is believed that their role in prevention of NHO is by inhibiting the mineralisation of organic osteoid.36,38 In addition to primary prevention, the question of bisphosphonate efficacy in secondary prevention and treatment of HO is an important one.39 Clinically significant HO has been shown to be prevented if therapy is initiated after bone scan evidence has been identified, but before findings of HO on plain films.35 Additionally, bisphosphonates may have long-term effects on prevention of significant HO years after they are discontinued.35 Unfortunately, additional musculoskeletal injuries are often co-morbid with spinal cord injury and traumatic brain injury and, therefore, the use of agents that inhibit new bone may impair fracture healing. To that effect, there is data to suggest that bisphosphonates delay callus remodeling in dogs.39 Given that nearly all of the spinal cord and traumatic brain injured patients we treat at our institution have significant orthopaedic injuries, we do not routinely use bisphosphonates for neurogenic HO prophylaxis or management.
Radiation
Radiation therapy (RT) is another treatment used in managing patients with HO and it is thought to work by preventing the differentiation of mesenchymal progentitor cells into HO-forming osteoblasts.40 RT may be given as primary or secondary prophylaxis.41 Primary prophylaxis is generally initiated in the severely injured patients in whom the risk of developing HO is thought to be substantial. In this setting RT is generally given peri-operatively. It has been well-established that single-fraction RT pre-operatively is equally as effective as multi-fractionated post-operative RT.42,43 Alternatively, RT may be given as secondary prophylaxis in those who have already been diagnosed with HO and are undergoing surgical resection.44
Radiation therapy has proven to be effective in preventing the formation of HO in patients undergoing surgery about the hip, whether total hip arthroplasty or open reduction and internal fixation.45 There is also evidence to support its use about the elbow, shoulder and knee.44 However, some authors have shown that single-fraction therapy administered to elbow fractures leads to an increase risk of nonunion.46 More research is needed in this area. The standard doses used in these patients however have proven to be ineffective in patients with NHO.45 In one trial specifically looking at NHO, single fractions of radiation were administered for a total dose of 10 Gy to 52 patients and 75 joints over a period of 11 years. A total of 58 joints received the radiation as primary treatment and the remaining 17 were treated following resection. For the analysis 49 patients were evaluated for a total of 70 joints, 65 of which were hips, with a mean follow-up of 11 months. Of the 70 joints, 50 (71%) showed no signs of HO progression.47 Another trial focused primarily on patients receiving RT following surgical resection of HO.47 The study comprised 33 patients, 30 of whom showed no progression of HO and improvements in mobilisation and rehabilitation. The remaining three patients experienced a moderate decrease in mobility and increase in their grade of HO.47
Physical therapy
The role of physical therapy in patients with HO is somewhat controversial. There are those who believe that aggressive ROM may lead to increase bone formation. Most, however, agree that physical therapy preserves movement, leading to better function and prevention of ankylosis.35,48,49 Physiotherapy typically involves active and passive ROM, gentle terminal stretch and resisted ROM exercise.
Surgery
The surgical management of HO aims to improve mobility and decrease the complications of immobility such as pressure ulcers, intractable pain and impingement of important neurovascular structures. In addition, surgery allows for the patient or the caretaker to improve mobility and ease of care. With any surgery it is paramount to have appropriate pre-operative planning before entering the operating room, in order to limit potential complications such as infection, fracture, recurrence and intra-operative bleeding.1,50,51 The baseline values of alkaline phosphatase, radiographs, 3D CT, and bone scan data should be considered (Fig. 3). These data are ultimately used to determine the timing of surgery, which has traditionally been recommended to take place one year following SCI for most patients and 1.5 years following TBI.52 These recommendations are based primarily on the usual time to radiological maturation that is seen with SCI and, in the case of TBI, the added time for motor recovery to occur. The purpose of waiting until maturity is to minimise the rate of recurrence following resection. This timing, however, does not always correlate with clinical necessity of resection and surgery may need to be considered sooner to manage difficult complications that can be seen with progressive HO.1 In these cases, earlier intervention may need to be considered with the understanding that increased complications (such as bleeding) may occur intra-operatively and recurrence is a possibility. However, recent data suggest that resection of immature HO may not necessarily have an increased rate of recurrence.53 Delaying surgical intervention may lead to irreversible joint injury. Further investigation is necessary to elucidate the importance of timing.
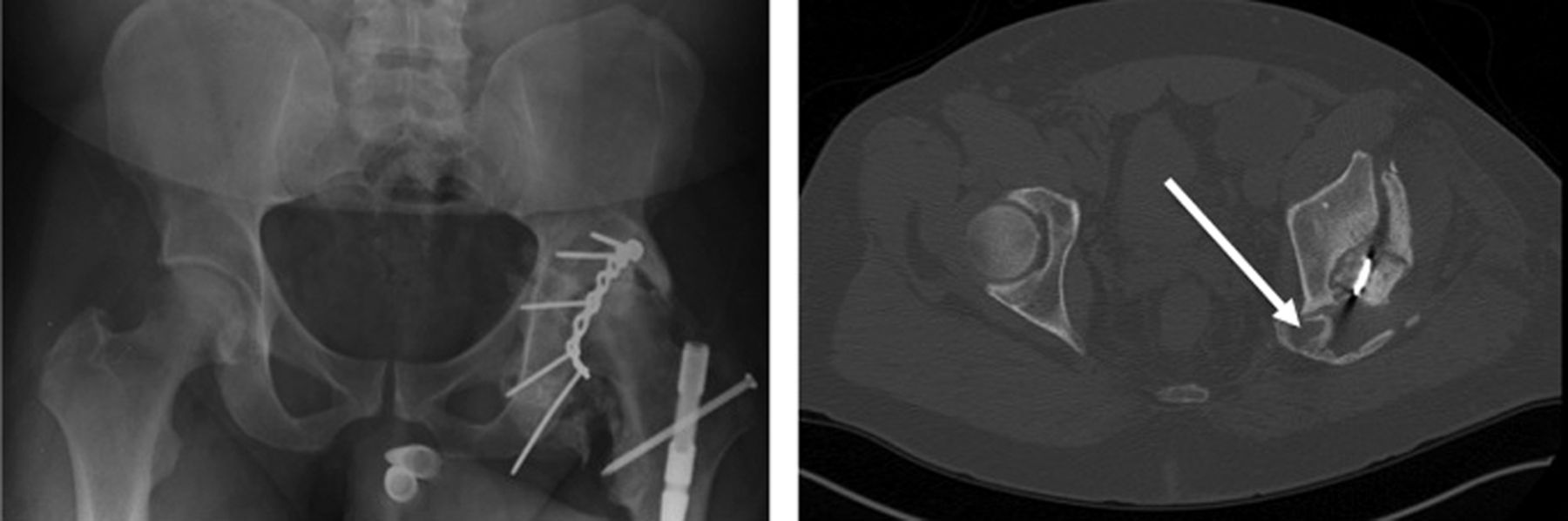
Fig. 3
A 37-year-old male patient sustained a fracture of the left acetabulum and traumatic brain injury after a high-speed automobile collision. The patient underwent open reduction and internal fixation of the left acetabular fracture within four days of the injury. Anteroposterior radiograph (left) and CT (right) were taken six months after injury and show the sciatic nerve encased in heterotopic bone (arrow). Advanced imaging was essential for diagnosis and pre-operative planning for surgical resection.
Patients being considered for surgery should also have an appropriate cognitive and physical function assessment. The excision of HO can provide significant improvements in ROM and, in appropriate patients, can be a successful operation with minimal complications. Patients with good neurological recovery and motor function are less likely to recur than those with severe motor and cognitive deficits.52 One case series evaluated 17 patients with 20 ankylosed joints (13 hips and seven elbows) with a mean follow-up of 23 months who underwent surgical resection and concomitant bisphosphonate therapy.54 The mean ROM achieved in the immediate post-operative period was 85° for the hips and 65° for the elbows. One hip and one elbow experienced recurrence at 11 months and 13 months post-operatively, respectively. Both of these patients had serious cognitive and physical disabilities. The remaining joints were able to maintain a functional ROM, although no specific values were cited.54 Another study investigated 29 patients undergoing HO resection about the hip with concomitant radiation and physical therapy, and found the ROM of the hips to be a mean of 94.5° immediately post-operatively, sustained to a mean of 82.7° at four years.51
Conclusion
Neurogenic heterotopic ossification is characterised by the formation of bone in soft tissues, especially around large joints, following traumatic injury to the central nervous system. The hip is the most commonly involved joint in both spinal cord injury and traumatic brain injury. The severity of disease ranges from asymptomatic radiological findings to complete joint ankylosis and fixed contractures. Early NHO is difficult to diagnose and may mimic other processes often seen in injured patients such as cellulitis, septic arthritis and phlebitis. This presentation may lead to delays in diagnosis increasing patient morbidity and subjecting the patient and health system to costly and invasive procedures. Once diagnosed, management of NHO presents unique challenges to the orthopaedic surgeon. Complications and recurrence rates are high and in general, severity of CNS injury negatively correlates with outcomes. NHO predisposes patients to UTI, pneumonia, pressure ulcers, pain, poor hygiene and loss of function. The literature suggests reasonably good results for primary and secondary prevention with NSAIDs, bisphosphonates and radiation. However, given the high rate of comorbid osseous and visceral injuries in the polytraumatised orthopaedic patient, these therapies require careful management or may be contraindicated. Surgical excision and joint release can provide improvements for many patients but have varied results and often depend on the degree of CNS injury.
1 Cipriano CA , PillSG, KeenanMA. Heterotopic ossification following traumatic brain injury and spinal cord injury. J Am Acad Orthop Surg2009;17:689–697.PubMed Google Scholar
2 Wittenberg RH , PeschkeU, BötelU. Heterotopic ossification after spinal cord injury: epidemiology and risk factors. J Bone Joint Surg [Br]1992;74-B:215–218. Google Scholar
3 van Kuijk AA , GeurtsAC, van KuppeveltHJ. Neurogenic heterotopic ossification in spinal cord injury. Spinal Cord2002;40:313–326.CrossrefPubMed Google Scholar
4 Simonsen LL , Sonne-HolmS, KrasheninnikoffM, EngbergAW. Symptomatic heterotopic ossification after very severe traumatic brain injury in 114 patients: incidence and risk factors. Injury2007;38:1146–1150.CrossrefPubMed Google Scholar
5 Vanden Bossche L , VanderstraetenG. Heterotopic ossification: a review. J Rehabil Med2005;37:129–136. Google Scholar
6 Genêt F , JourdanC, SchnitzlerA, et al.Troublesome heterotopic ossification after central nervous system damage: a survey of 570 surgeries. PloS One2011;6:16632.CrossrefPubMed Google Scholar
7 Genêt F , JourdanC, LautridouC, et al.The impact of preoperative hip heterotopic ossification extent on recurrence in patients with head and spinal cord injury: a case control study. PloS One2011;6:23129.CrossrefPubMed Google Scholar
8 Larson JM , MichalskiJP, CollacottEA, et al.Increased prevalence of HLA-B27 in patients with ectopic ossification following traumatic spinal cord injury. Rheumatol Rehabil1981;20:193–197.CrossrefPubMed Google Scholar
9 Garland DE , AldayB, VenosKG. Heterotopic ossification and HLA antigens. Arch Phys Med Rehabil1984;65:531–532.PubMed Google Scholar
10 Garland DE . Clinical observations on fractures and heterotopic ossification in the spinal cord and traumatic brain injured populations. Clin Orthop Relat Res1988;233:86–101.PubMed Google Scholar
11 Chalidis B , StengelD, GiannoudisPV. Early excision and late excision of heterotopic ossification after traumatic brain injury are equivalent: a systematic review of the literature. J Neurotrauma2007;24:1675–1686.CrossrefPubMed Google Scholar
12 Ebinger T , RoeschM, KieferH, KinzlL, SchulteM. Influence of etiology in heterotopic bone formation of the hip. J Trauma2000;48:1058–1062.CrossrefPubMed Google Scholar
13 Garland DE , O’HollarenRM. Fractures and dislocations about the elbow in the head-injured adult. Clin Orthop Relat Res1982;168:38–41.PubMed Google Scholar
14 Halas RA , KaruppiahS. Heterotopic ossification of the hip after stroke. Curr Orthop Pract2011;22:E19–E21. Google Scholar
15 Kurer MH , KhokerMA, DandonaP. Human osteoblast stimulation by sera from paraplegic patients with heterotopic ossification. Paraplegia1992;30:165–168.CrossrefPubMed Google Scholar
16 Cooper RR , MilgramJW, RobinsonRA. Morphology of the osteon: an electron microscopic study. J Bone Joint Surg [Am]1966;48-A:1239–1271. Google Scholar
17 Bidner SM , RubinsIM, DesjardinsJV, ZukorDJ, GoltzmanD. Evidence for a humoral mechanism for enhanced osteogenesis after head injury. J Bone Joint Surg [Am]1990;72-A:1144–1149.PubMed Google Scholar
18 Kim JS , YoonSS, KimYH, RyuJS. Serial measurement of interleukin-6, transforming growth factor-beta, and S-100 protein in patients with acute stroke. Stroke1996;27:1553–1557.CrossrefPubMed Google Scholar
19 Pasinetti GM , NicholsNR, ToccoG, et al.Transforming growth factor beta 1 and fibronectin messenger RNA in rat brain: responses to injury and cell-type localization. Neuroscience1993;54:893–907.CrossrefPubMed Google Scholar
20 Cadosch D , GautschiOP, ThyerM, et al.Humoral factors enhance fracture-healing and callus formation in patients with traumatic brain injury. J Bone Joint Surg [Am]2009;91-A:282–288.CrossrefPubMed Google Scholar
21 Cadosch D , ToffoliAM, GautschiOP, et al.Serum after traumatic brain injury increases proliferation and supports expression of osteoblast markers in muscle cells. J Bone Joint Surg [Am]2010;92-A:645–653.CrossrefPubMed Google Scholar
22 Hohmann EL , EldeRP, RysavyJA, EinzigS, GebhardRL. Innervation of periosteum and bone by sympathetic vasoactive intestinal peptide-containing nerve fibers. Science1986;232:868–871.CrossrefPubMed Google Scholar
23 Jones KB , MollanoAV, MorcuendeJA, CooperRR, SaltzmanCL. Bone and brain: a review of neural, hormonal, and musculoskeletal connections. Iowa Orthop J2004;24:123–132.PubMed Google Scholar
24 Argyropoulou MI , KostandiE, KostaP, et al.Heterotopic ossification of the knee joint in intensive care unit patients: early diagnosis with magnetic resonance imaging. Crit Care2006;10:R152.CrossrefPubMed Google Scholar
25 Takeda S , ElefteriouF, LevasseurR, et al.Leptin regulates bone formation via the sympathetic nervous system. Cell2002;111:305–317.CrossrefPubMed Google Scholar
26 Wang L , TangX, ZhangH, et al.Elevated leptin expression in rat model of traumatic spinal cord injury and femoral fracture. J Spinal Cord Med2011;34:501–509.CrossrefPubMed Google Scholar
27 Kaplan FS , GlaserDL, HebelaN, ShoreEM. Heterotopic ossification. J Am Acad Orthop Surg2004;12:116–125.PubMedCrossref Google Scholar
28 Genet F , MarmoratJL, LautridouC, et al.Impact of late surgical intervention on heterotopic ossification of the hip after traumatic neurological injury. J Bone Joint Surg [Br]2009;91-B:1493–1498.CrossrefPubMed Google Scholar
29 Banovac K , WilliamsJM, PatrickLD, HaniffYM. Prevention of heterotopic ossification after spinal cord injury with indomethacin. Spinal Cord2001;39:370–374.CrossrefPubMed Google Scholar
30 Banovac K , WilliamsJM, PatrickLD, LeviA. Prevention of heterotopic ossification after spinal cord injury with COX-2 selective inhibitor (rofecoxib). Spinal Cord2004;42:707–710.CrossrefPubMed Google Scholar
31 United States Food and Drug Administration. FDA News Release P04-95, September 2004. http://www.fda.gov/NewsEvents/Newsroom/PressAnnouncements/2004/ucm108361.htm (date last accessed 4 March 2013). Google Scholar
32 Francis MD , RussellRG, FleischH. Diphosphonates inhibit formation of calcium phosphate crystals in vitro and pathological calcification in vivo. Science1969;165:1264–1266.CrossrefPubMed Google Scholar
33 Finerman GA , StoverSL. Heterotopic ossification following hip replacement or spinal cord injury: two clinical studies with EHDP. Metab Bone Dis Relat Res1981;3:337–342. Google Scholar
34 Stover SL , HahnHR, MillerJM. Disodium etidronate in the prevention of heterotopic ossification following spinal cord injury (preliminary report). Paraplegia1976;14:146–156.CrossrefPubMed Google Scholar
35 Banovac K . The effect of etidronate on late development of heterotopic ossification after spinal cord injury. J Spinal Cord Med2000;23:40–44.CrossrefPubMed Google Scholar
36 Banovac K , GonzalezF, WadeN, BowkerJJ. Intravenous disodium etidronate therapy in spinal cord injury patients with heterotopic ossification. Paraplegia1993;31:660–666.CrossrefPubMed Google Scholar
37 Russell RG . Bisphosphonates: the first 40 years. Bone2011;49:2–19.CrossrefPubMed Google Scholar
38 Morris CD , EinhornTA. Bisphosphonates in orthopaedic surgery. J Bone Joint Surg [Am]2005;87-A:1609–1618.CrossrefPubMed Google Scholar
39 Peter CP , CookWO, NunamakerDM, et al.Effect of alendronate on fracture healing and bone remodeling in dogs. J Orthop Res1996;14:74–79.CrossrefPubMed Google Scholar
40 Sautter-Bihl ML , LiebermeisterE, NanassyA. Radiotherapy as a local treatment option for heterotopic ossifications in patients with spinal cord injury. Spinal Cord2000;38:33–36.CrossrefPubMed Google Scholar
41 Balboni TA , GobezieR, MamonHJ. Heterotopic ossification: pathophysiology, clinical features, and the role of radiotherapy for prophylaxis. Int J Radiat Oncol Biol Phys2006;65:1289–1299.CrossrefPubMed Google Scholar
42 Seegenschmiedt MH , MartusP, GoldmannAR, et al.Preoperative versus postoperative radiotherapy for prevention of heterotopic ossification (HO): first results of a randomized trial in high-risk patients. Int J Radiat Oncol Biol Phys1994;30:63–73.CrossrefPubMed Google Scholar
43 Seegenschmiedt MH , KeilholzL, MartusP, et al.Prevention of heterotopic ossification about the hip: final results of two randomized trials in 410 patients using either preoperative or postoperative radiation therapy. Int J Radiat Oncol Biol Phys1997;39:161–171. Google Scholar
44 Mishra MV , AustinL, ParviziJ, RamseyM, ShowalterTN. Safety and efficacy of radiation therapy as secondary prophylaxis for heterotopic ossification of non-hip joints. J Med Imaging Radiat Oncol2011;55:333–336.CrossrefPubMed Google Scholar
45 Cipriano C, Pill SG, Rosenstock J, Keenan MA. Radiation therapy for preventing recurrence of neurogenic heterotopic ossification. Orthopedics 2009;32. Google Scholar
46 Hamid N , AshrafN, BosseMJ, et al.Radiation therapy for heterotopic ossification prophylaxis acutely after elbow trauma: a prospective randomized study. J Bone Joint Surg [Am]2010;92-A:2032–2038.CrossrefPubMed Google Scholar
47 Sautter-Bihl ML , HültenschmidtB, LiebermeisterE, NanassyA. Fractionated and single-dose radiotherapy for heterotopic bone formation in patients with spinal cord injury: a phase-I/II study. Strahlenther Onkol2001;177:200–205. Google Scholar
48 Stover SL , HatawayCJ, ZeigerHE. Heterotopic ossification in spinal cord-injured patients. Arch Phys Med Rehabil1975;56:199–204.PubMed Google Scholar
49 Garland DE , RazzaBE, WatersRL. Forceful joint manipulation in head-injured adults with heterotopic ossification. Clin Orthop Relat Res1982;169:133–138.PubMed Google Scholar
50 Garland DE , HanscomDA, KeenanMA, SmithC, MooreT. Resection of heterotopic ossification in the adult with head trauma. J Bone Joint Surg [Am]1985;67-A:1261–1269.PubMed Google Scholar
51 Meiners T , AbelR, BohmV, GernerHJ. Resection of heterotopic ossification of the hip in spinal cord injured patients. Spinal Cord1997;35:443–445.CrossrefPubMed Google Scholar
52 Garland DE , OrwinJF. Resection of heterotopic ossification in patients with spinal cord injuries. Clin Orthop Relat Res1989;242:169–176.PubMed Google Scholar
53 Freebourn TM , BarberDB, AbleAC. The treatment of immature heterotopic ossification in spinal cord injury with combination surgery, radiation therapy and NSAID. Spinal Cord1999;37:50–53.CrossrefPubMed Google Scholar
54 Moore TJ . Functional outcome following surgical excision of heterotopic ossification in patients with traumatic brain injury. J Orthop Trauma1993;7:11–14.CrossrefPubMed Google Scholar
Funding statement:
None declared
Author contributions:
M. P. Sullivan: Principal co-author: formal manuscript draft preparation, relevant literature search and review
S. J. Torres: Principal co-author: formal manuscript draft preparation, relevant literature search and review
S. Mehta: Senior author: reviewed and edited manuscript repeatedly including final manuscript draft
J. Ahn: Senior author: formulated manuscript outline, reviewed and edited manuscript repeatedly including final manuscript draft
ICMJE Conflict of Interest:
None declared
©2013 The British Editorial Society of Bone & Joint Surgery. This is an open-access article distributed under the terms of the Creative Commons Attributions licence, which permits unrestricted use, distribution, and reproduction in any medium, but not for commercial gain, provided the original author and source are credited.
