




Abstract
Aims
Approved by the Food and Drug Administration in 2004, the Phase III Oxford Medial Partial Knee is used to treat anteromedial osteoarthritis (AMOA) in patients with an intact anterior cruciate ligament. This unicompartmental knee arthroplasty (UKA) is relatively new in the United States, and therefore long-term American results are lacking.
Patients and Methods
This is a single surgeon, retrospective study based on prospectively collected data, analysing a consecutive series of primary UKAs using the Phase III mobile-bearing Oxford Knee and Phase III instrumentation.
Between July 2004 and December 2006, the senior author (RHE) carried out a medial UKA in 173 patients (213 knees) for anteromedial osteoarthritis or avascular necrosis (AVN).
A total of 95 patients were men and 78 were women. Their mean age at surgery was 67 years (38 to 89) and mean body mass index 29.87 kg/m2 (17 to 62).
The mean follow-up was ten years (4 to 11).
Results
Survivorship of the Oxford UKA at ten years was 88%, using life table analysis. Implant survivorship at ten years was 95%. The most common cause for revision was the progression of osteoarthritis in the lateral compartment. The mean knee score element of the American Knee Society Score (AKSS) was 50 pre-operatively and increased to 93 post-operatively. The mean AKSS function score was 56 pre-operatively rising to 78 post-operatively
Conclusion
This ten-year follow-up study of the Oxford UKA undertaken in the United States shows good survivorship and excellent function in a wide selection of patients with AMOA and AVN.
Cite this article: Bone Joint J 2016;98-B(10 Suppl B):34–40.
The Oxford unicompartmental knee arthroplasty (UKA) is primarily indicated for patients with anteromedial osteoarthritis (AMOA) of the knee.1 AMOA with a functionally intact anterior cruciate ligament (ACL), is a clinicopathological entity characterised by a specific wear pattern of cartilage and bone erosion limited to the anterior and centromedial compartment of the knee. Knees with AMOA tend to be in varus alignment and are not painful in flexion because the posterior elements of the joint are preserved, consequently protecting the medial collateral ligament (MCL) from shortening.1
This study is a longitudinal follow-up of a consecutive series of medial UKAs. It aims to determine the survivorship of the implant and patient-reported outcomes. It also proposes criteria for the appropriate selection of patients for UKA and provides an in-depth analysis of revision cases. It is the first ten-year follow-up of a mobile-bearing medial UKA undertaken in the United States since the Food and Drug Administration (FDA) approved the device in 2004.
Patients and Methods
This is a retrospective review of prospectively collected data in a practice-based registry. Patients were followed-up at six weeks, six months, one year, and every two years after the first post-operative year.
Between July 2004 and December 2006, the senior author (RHE) carried out 213 consecutive primary medial UKAs in 173 patients using the Phase III mobile-bearing cemented Oxford Knee (Zimmer Biomet, Warsaw, Indiana), Phase III instrumentation and a minimally invasive surgical approach. There were 95 men and 78 women in the series. Their mean age at surgery was 67 years (38 to 89) and mean body mass index (BMI) 30 kg/m2 (17 to 62).
Follow-up consisted of establishing the American Knee Society Score (AKSS) and obtaining anteroposterior and lateral radiographs. Range of movement (ROM) was assessed with the patient supine, measuring from the lateral side by placing a 12-inch goniometer in a line from the greater trochanter to the lateral femoral condyle and thence to lateral malleolus.2
The AKSS is a validated total knee rating system. It is subdivided into a knee score which rates the knee joint, and a functional score which rates the patient’s ability to walk and climb stairs (both scores have a maximum of 100 points).3 The pre-operative score closest to surgery and the most recent post-operative score were used in each case in this study. Patients who had not completed a recent follow-up visit were contacted by phone and were asked AKSS questions related to pain, function, and status of the implant. In order to determine the status of deceased patients’ implants, their most recent hospital and clinical records were obtained. Evidence of the implant label, to ensure that an Oxford UKA had been implanted, as well as patient confirmation of implant status, were required to establish survivorship.
The primary indications for Oxford UKA are patients with AMOA; bone-on-bone medially; intact anterior cruciate and collateral ligaments; a correctable varus deformity; asymptomatic or absent patellofemoral disease and full cartilage thickness laterally. Secondary indications are osteonecrosis or avascular necrosis (AVN) limited to the medial compartment. Contraindications previously described by Kozinn and Scott4 (age, BMI, activity level, chondrocalcinosis, etc.) were not considered to be contraindications. Absolute contraindications are lateral compartment disease; symptomatic patellofemoral disease; ligament instability, excessive flexion contracture, and the presence of any infection or inflammatory disease. Patellofemoral arthritis limited to the medial side was not considered a contraindication, although if present on the lateral side, was deemed to be so. The final decision to carry out a UKA was made intra-operatively after verifying the integrity of the ACL and the lateral tibiofemoral compartment.
Statistical analysis
A survival analysis was undertaken using the life table method for various definitions of failure.5
UKA survivorship considered all revisions as the end point, regardless of cause. Revisions were defined as any replacement of components. Implant survivorship did not include revisions at which the original Oxford implant was determined to be well fixed and functional (confirmed from the operating record), but was nonetheless revised either because of lateral compartmental osteoarthritis (LCOA) or haemarthrosis. The 95% confidence intervals (CI) were calculated using the Peto method.6 Statistical analysis and graphs were prepared using Microsoft Excel (Microsoft, Redmond, Washington) macros.
Results
The mean follow-up was ten years (4 to 11). Patient contact was attempted by phone and mail. Of the 173 patients (213 knees), nine patients (11 knees 5%) died and 21 patients (34 knees 16%) were lost to follow-up. None of the deaths were related to the implant or surgical complications. The survivorship of the UKA at ten years was 88% (95% CI 5.6) (Fig. 1, Table I) and implant survivorship (95% CI 3.8) (Fig. 2, Table II).
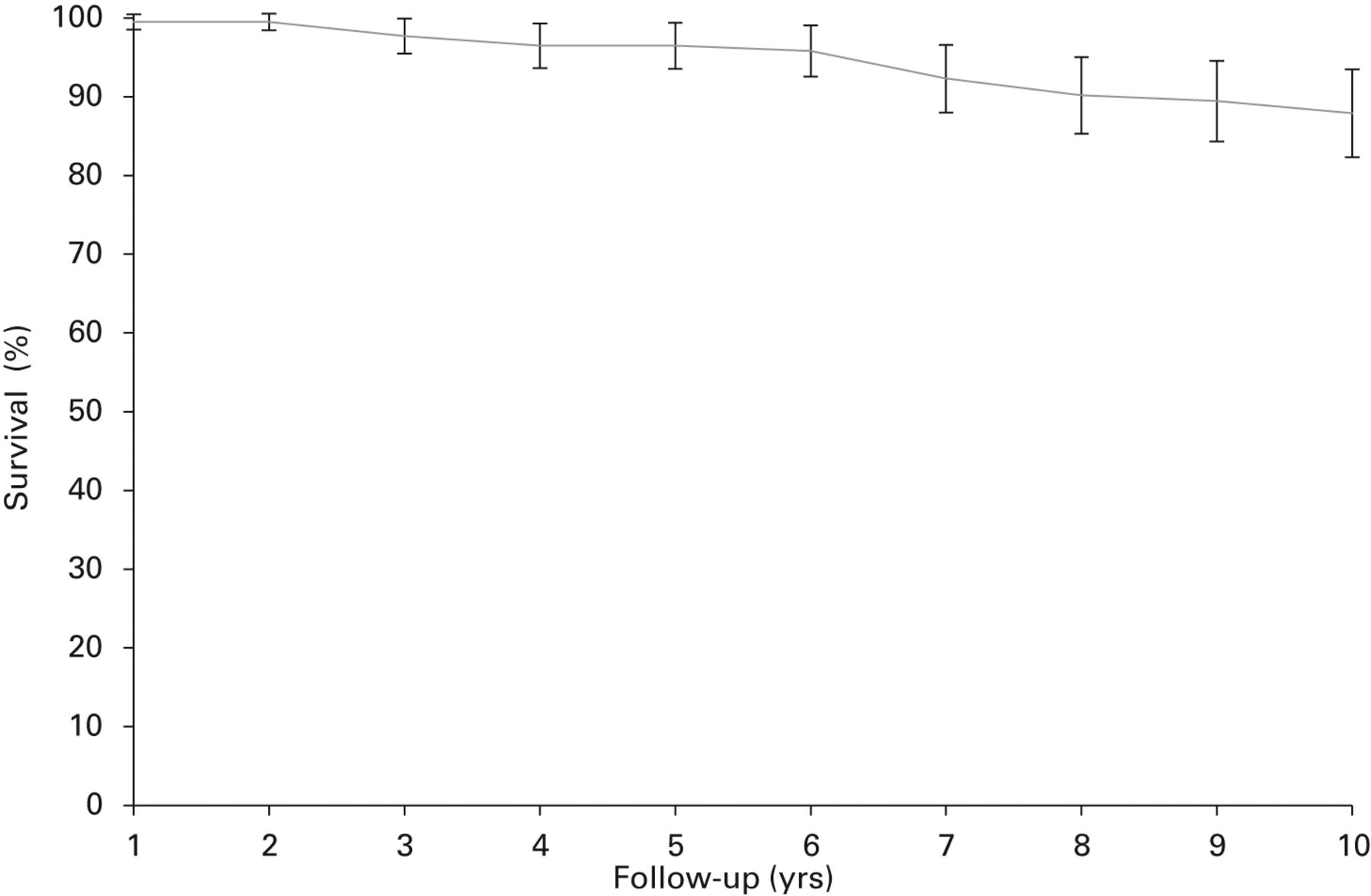
Fig. 1
Unicompartmental knee arthroplasty (UKA) survivorship at ten years - survival curve showing survival of the minimally invasive Oxford phase III UKA with all revisions as the end point.
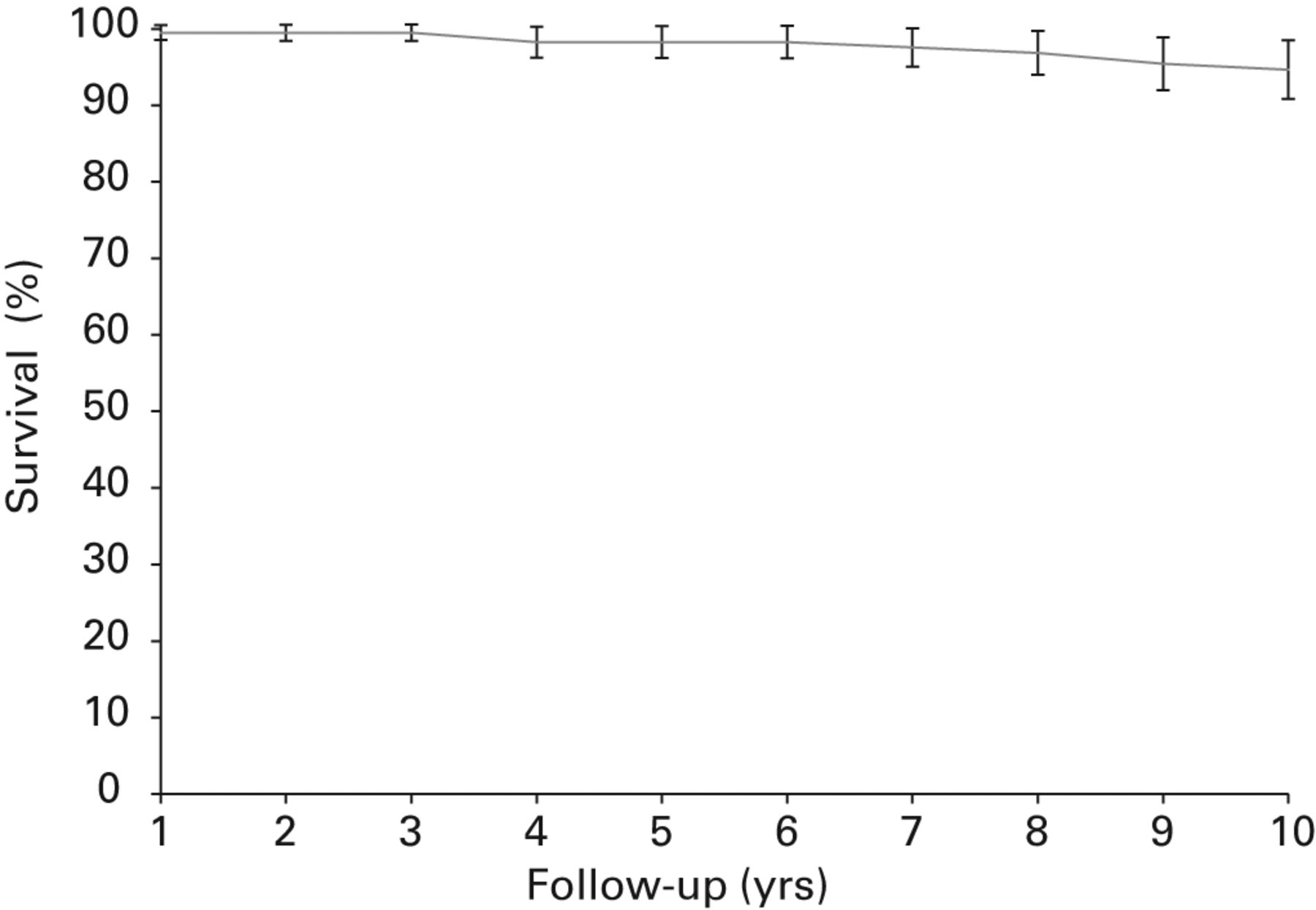
Fig. 2
Implant survivorship at 10 years - survival curve showing survival of the minimally Oxford phase III unicompartmental knee arthroplasty with non-implant related revisions as the endpoint.
Table I
Life table for all 213 unicompartmental knee arthroplasties with implant-related revisions as the endpoint. Lost to follow-up (LTF), revision rate (Rev rate), success rate (Suc rate), survivorship percentage (% Surv)
| Yrs | n | Revised | Deaths | LTF | n (at risk) | Rev rate | Suc rate | % Surv | 95% CI |
|---|---|---|---|---|---|---|---|---|---|
| 1 | 213 | 1 | 0 | 30 | 198 | 0.01 | 0.99 | 99.5 | 1.0 |
| 2 | 182 | 0 | 1 | 12 | 175.5 | 0.00 | 1.00 | 99.5 | 1.0 |
| 3 | 169 | 3 | 0 | 4 | 167 | 0.02 | 0.98 | 97.7 | 2.2 |
| 4 | 162 | 2 | 0 | 8 | 158 | 0.01 | 0.99 | 96.5 | 2.8 |
| 5 | 152 | 0 | 0 | 9 | 147.5 | 0.00 | 1.00 | 96.5 | 2.9 |
| 6 | 143 | 1 | 2 | 2 | 141 | 0.01 | 0.99 | 95.8 | 3.2 |
| 7 | 138 | 5 | 0 | 2 | 137 | 0.04 | 0.96 | 92.3 | 4.3 |
| 8 | 131 | 3 | 1 | 1 | 130 | 0.02 | 0.98 | 90.2 | 4.9 |
| 9 | 126 | 1 | 0 | 4 | 124 | 0.01 | 0.99 | 89.4 | 5.1 |
| 10 | 121 | 2 | 5 | 6 | 115.5 | 0.02 | 0.98 | 87.9 | 5.6 |
Table II
Life table for all 213 unicompartmental knee arthroplasties with non-implant-related revisions as the endpoint. Lost to follow-up (LTF), revision rate (Rev rate), success rate (Suc rate), survivorship percentage (% Surv)
| Yrs | n | Revised | Deaths | LTF | n (at risk) | Rev rate | Suc rate | % Surv | 95% CI |
|---|---|---|---|---|---|---|---|---|---|
| 1 | 213 | 1 | 0 | 30 | 198 | 0.01 | 0.99 | 99.5 | 1.0 |
| 2 | 182 | 0 | 1 | 12 | 175.5 | 0.00 | 1.00 | 99.5 | 1.0 |
| 3 | 169 | 0 | 0 | 4 | 167 | 0.00 | 1.00 | 99.5 | 1.1 |
| 4 | 165 | 2 | 0 | 8 | 161 | 0.01 | 0.99 | 98.3 | 2.0 |
| 5 | 155 | 0 | 0 | 9 | 150.5 | 0.00 | 1.00 | 98.3 | 2.1 |
| 6 | 146 | 0 | 2 | 2 | 144 | 0.00 | 1.00 | 98.3 | 2.1 |
| 7 | 142 | 1 | 0 | 2 | 141 | 0.01 | 0.99 | 97.6 | 2.5 |
| 8 | 139 | 1 | 1 | 1 | 138 | 0.01 | 0.99 | 96.9 | 2.9 |
| 9 | 136 | 2 | 0 | 4 | 134 | 0.01 | 0.99 | 95.4 | 3.5 |
| 10 | 130 | 1 | 5 | 6 | 124.5 | 0.01 | 0.99 | 94.6 | 3.8 |
Patients exhibited a good ROM post-operatively, with a mean 0.42° of extension (-10° to 10°) and 123° of flexion (90° to 140°). A total of 159 patients had an excellent post-operative AKSS knee score with six good, five fair and five poor results. The mean pre-operative AKSS knee score was 50 and rose to 93 post-operatively (0 to 95 and 0 to 100, respectively). The mean pre-operative AKSS function score was 56 and rose to 78 post-operatively (0 to 100 and -10 to 100, respectively) (Fig. 3). The mean AKSS follow-up for scores is eight years (0.5 to 11). A total of five patients (six knees) were followed-up until their recent death, and reported a mean Knee Score of 98, and a mean Knee Function Score of 88 (93 to 100 and 45 to 100, respectively).
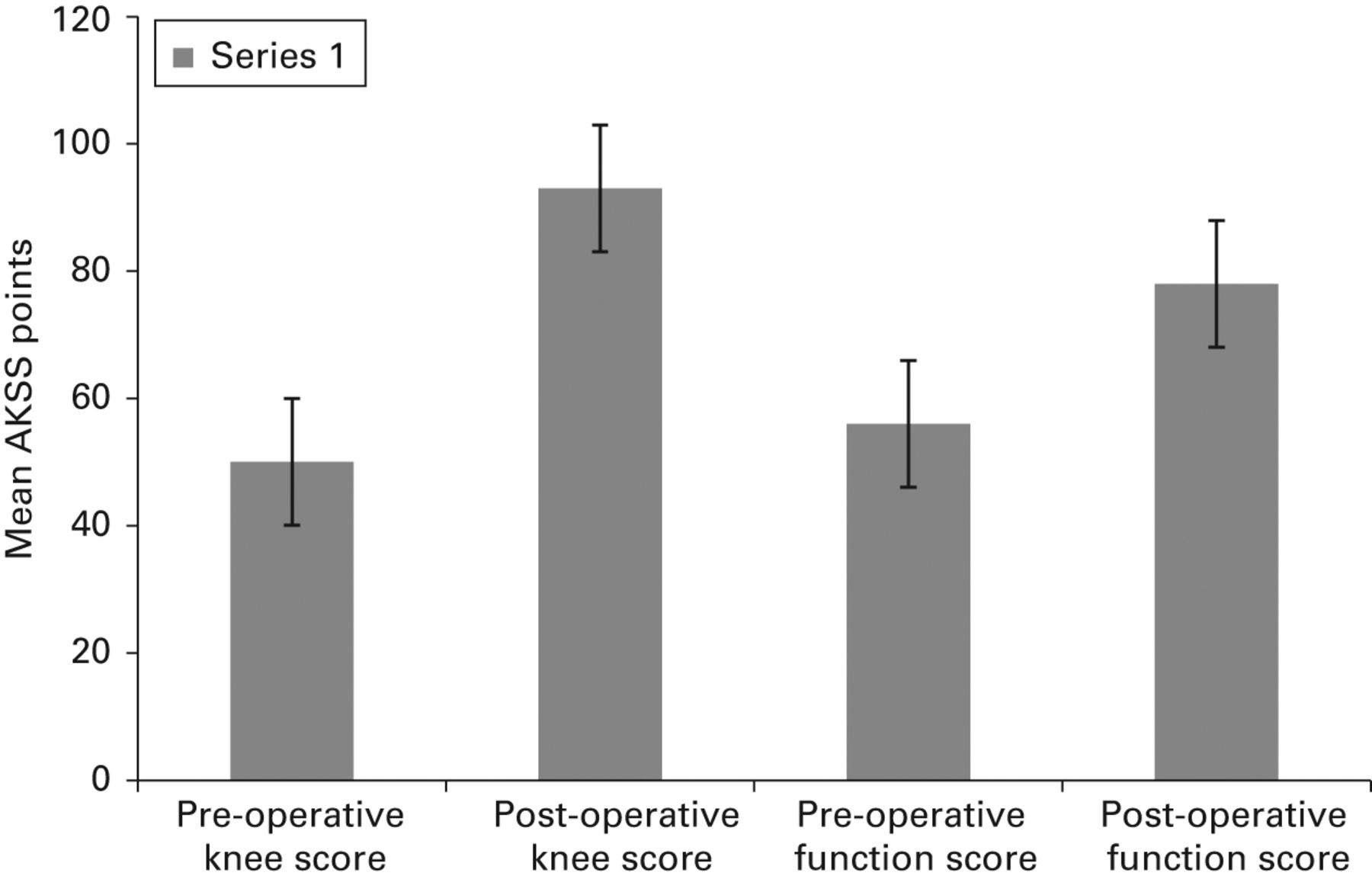
Fig. 3
American Knee Society Score (AKSS) pre- and post-operative scores - clinical outcomes (mean,sd error bars). AKSS Knee and function scores displayed. The mean AKSS follow-up for scores is 8 years (0.5 to 11).
Revisions
A total of 20 patients (20 knees; 9.4%) were revised in this study at a mean of 6.2 years (2 to 11) after Oxford UKA (Table III). The mean BMI of patients revised was 29 kg/m2 (19 to 49), which is slightly lower than the overall mean patient BMI. Most revisions, 4.2% of all implanted Oxfords, were due to the progression of LCOA. One patient with LCOA ten years post Oxford UKA, had a well-fixed medial Oxford UKA, and was treated with the addition of a lateral UKA, and reported good outcomes through the first post-operative year (Knee Function Score 80, Knee Score 90).
Table III
Details of the 20 revisions
| Patient | Time to revision (yrs) | Reason for revision | Operative findings | Revision and outcome |
|---|---|---|---|---|
| 1 | 0.73 | Loose tibial component | Micromotion seen in the tibial aspect of the tibia, loose tibial component. | Revised to TKA, Vanguard CR* |
| 2 | 2.1 | Chronic haemarthrosis | Fresh blood discovered in the knee, full thickness cartilage loss on the trochlea and lateral compartment. | Revised to TKA, Vanguard CR |
| 3 | 2.6 | Chronic haemarthrosis | Progressive cartilage loss in lateral compartment, 200ml of fresh blood in joint, boggy synovium, Oxford in good position and bearing was tracking. | Revised to TKA, Vanguard CR* |
| 4 | 2.7 | Progression of osteoarthritis in the lateral compartment | Lupus arthritis progression into lateral compartment, original oxford components were well fixed and aligned. | Revised to TKA, Vanguard CR* |
| 5 | 3 | Unknown, revised elsewhere | Unknown | Revised to TKA |
| 6 | 3.7 | Progression of osteoarthritis in the lateral compartment | Significant arthritic erosive changes to lateral femoral condyle, previous components in please with no loosening. | Revised to TKA, Zimmer* |
| 7 | 3.7 | Progression of osteoarthritis in the lateral compartment | Progression of osteoarthritis in the lateral compartment | Revised to TKA, done elsewhere |
| 8 | 5.9 | Progression of osteoarthritis in the lateral compartment | Bone on bone lateral degenerative joint disease, Oxford components were well fixed and functioning well. | Revised to TKA, Vanguard CR* |
| 9 | 6 | Bearing dislocation | Posterior displacement of bearing. | Bearing change to thicker bearing. |
| 10 | 6.1 | Progression of osteoarthritis in the lateral compartment | Inflammatory synovitis with cartilage disease progress. | Revised to TKA, Vanguard CR |
| 11 | 6.3 | Progression of osteoarthritis in the lateral compartment | Progression of osteoarthritis in the lateral compartment | Revised to TKA, done elsewhere |
| 12 | 6.5 | Progression of osteoarthritis in the lateral compartment | Bone on bone lateral degenerative joint disease, Oxford components were well fixed and functioning well. | Revised to TKA, Vanguard PS* |
| 13 | 6.9 | Progression of osteoarthritis in the lateral compartment | Bone on bone lateral degenerative joint disease, Oxford components were well fixed and functioning well. | Revised to TKA, Vanguard CR* |
| 14 | 7.1 | Chronic haemarthrosis | Progressive cartilage loss in lateral compartment, 200 ml of fresh blood in joint, Oxford in good position and bearing was tracking. | Revised to TKA, Vanguard CR* |
| 15 | 7.7 | Unknown, revised elsewhere | Unknown | Revised to TKA, done elsewhere |
| 16 | 8.1 | Loose tibial component | Loose tibial component, lateral compartment showed no signs of wear. | Revised to TKA, Vanguard PS |
| 17 | 9.5 | Loose femoral component | Femoral component loose | Revised to TKA, DJO Stemmed† femur and tibia revision system (RDR) |
| 18 | 9.8 | Polyethylene Wear | Catastrophic failure of the bearing. | Revised to TKA, DJO Stemmed† femur and tibia revision system (RDR) |
| 19 | 11 | Progression of osteoarthritis in the lateral compartment | Bone on bone lateral degenerative joint disease, Oxford components were well fixed and functioning well. | Revised to TKA, Vanguard CR* |
| 20 | 11 | Loose femoral component | Femoral component loose | Revised to TKA, DJO Stemmed† femur and tibia revision system (RDR) |
-
* Zimmer Biomet, Warsaw, Indiana † DJO Global, Vista, California TKA, total knee arthroplasty
All patients who underwent revision were converted to a primary total knee arthroplasty (TKA), except for three patients treated elsewhere in whom stemmed revision components were used, and one whose posteriorly dislocated bearing was revised to a thicker bearing.
We found more revisions in patients with larger bearings (Fig. 4). One was attributed to impingement-related polyethylene wear. All bearing-related revisions, for dislocation or wear, had bearings of 5 mm or thicker. Of the nine bearings in which lateral compartment disease had progressed, three were 3 mm and six were 5 mm or more in thickness.
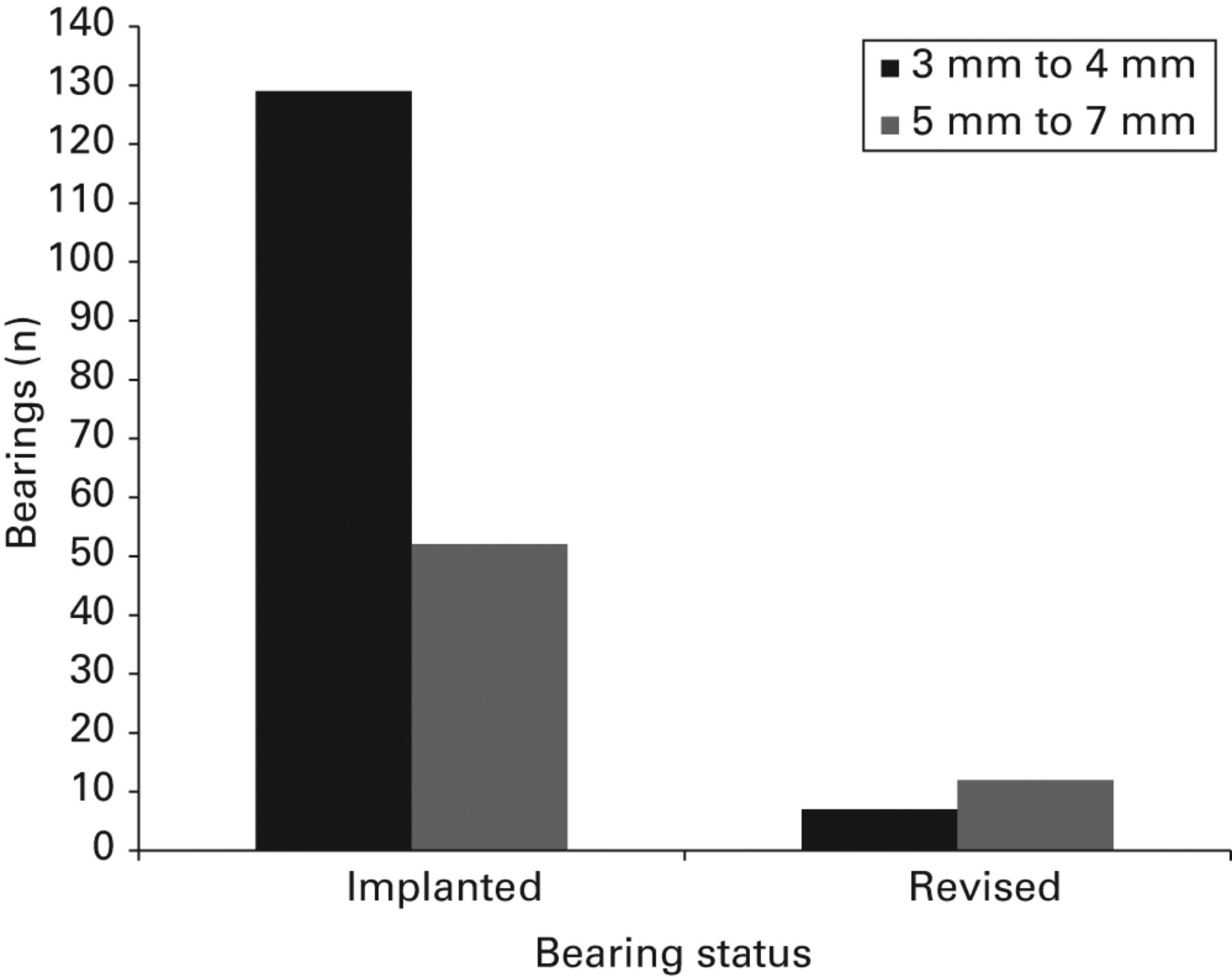
Fig. 4
Bearing thickness implanted versus revised: bar chart demonstrating total number of bearings implanted and revised, for thin (3 mm to 4 mm) and thick (5 mm to 7 mm) bearings.
Component loosening (four cases; two from the tibia and two from the femur) occurred in 1.9% of the knees in our study. Haemarthrosis-related revisions occurred in three patients (1.4%). Their intra-operative findings showed the tibial and femoral components were well fixed, but there was evidence of hypertrophic synovitis and extensive cartilage staining with haemosiderin and cartilage degeneration. These patients were initially treated conservatively. Several aspirations were undertaken to alleviate pain, none of which contained any signs of infection. There was no evidence of impingement.
Discussion
The clinical outcomes in this study were comparable with those from other Oxford UKA series. Price et al,7 Pandit et al,8 Kort et al,9 Rajasekhar, Das and Smith,10 and Kim et al11all reported a similar improvement in clinical scores. The improvements in ROM in this study (123.4° of maximum flexion) were comparable with those in other studies (Heller et al:12 123°, Kort et al:9 126.1°, Price et al:7 116°, Kristensen, Holm and Varnum:13 127.5°).
BMI did not seem to affect survivorship. This study provides further evidence that obesity is not a contraindication to Oxford UKA.14
The most common cause of revision in this study was LCOA. This is consistent with other reports.9,13,15,16 It highlights the importance of selecting patients with a normal lateral compartment at the time of primary surgery. Often, when lateral compartment osteoarthritis supervenes, the medial implant is well-fixed and well-functioning. ‘Addition of a lateral UKA’ (AOLU) is one method of addressing this. Pandit et al7 states that 13.8% of all revisions out of a series of 1000 Phase III Oxford UKA were treated with an AOLU, which gave good results beyond two years. In a study of lateral UKA to treat progressive arthritis after medial UKA, Pandit et al7 reported 100% survivorship in 27 knees after five years using this approach.17 Treating the progression of LCOA after Oxford UKA, with AOLU rather than TKA has several benefits, which include a quicker recovery, minimal soft-tissue or bony damage, and a shorter hospital stay. Historically, the first partial knee implants (1976 to 1982) were actually used bi-compartmentally as a total joint replacement, with two sets of components inserted, one medially and one laterally (Phase I Oxford).18
Svärd et al19 found no difference in survival between UKA and different thicknesses of bearing. However, others have correlated thicker bearings with a poorer clinical outcome. Lombardi et al20 found that their results were substantially better with a 3 mm or 4 mm bearing (94% 15-year survival) compared with one of 5 mm or more (75% 15-year survival). Dervin et al21found that overstuffing the medial compartment with a bearing that was too large resulted in overcorrection of the varus deformity and stressed the lateral compartment, inducing the progression of osteoarthritis. Pandit et al22 also found that an increased thickness of bearing was associated with significantly poorer results, and correlated a thicker bearing with a deeper tibial cut or an injury to the MCL. The Phase III instrumentation used in this series allowed for different amounts of tibial bone to be resected based on the surgeon’s preference, resulting in possible excessive removal of tibial bone. The current microplasty instrumentation provides for more reproducible and more conservative tibial cuts23 to accommodate the thinnest size 3 mm or 4 mm bearing.24
Recurrent haemarthrosis, considered to be recurrent after two consecutive episodes, was also reported as an indication for revision of an Oxford UKA by Zermatten et al,25 but appears to be a rare complication of knee arthroplasty and is mostly reported as individual cases.24,26-29 Recurrent haemarthrosis is more dangerous after a partial knee arthroplasty than after a TKA as normal articular cartilage has been retained. This can be damaged by bleeding, much as in the case of haemophiliac arthrosis. Data generated from pathophysiological research of osteoarthritis and rheumatoid arthritis suggests that multiple constituents in the blood trigger the process, and several joint components (articular cartilage, synovial membrane, blood vessels, and bone cells) are the targets.30 Structural joint damage can occur after just a few haemarthroses.30 There are a number of ways to treat this including open synovectomy,26 radiosynovectomy,24 interventional embolisation,28,29 and diagnostic arthroscopy.31
One failure in our series was due to anterior impingement-related polyethylene wear, which highlights the importance of removing impinging bone at the time of surgery. This is confirmed by a retrieval study conducted by Kendrick et al,32 in which it was concluded that the rate of polyethylene wear is increased if the bearings impinge on bone or cement. If there is no impingement, the rate of wear is very low (0.003 mm/year). The improved microplasty instrumentation has addressed the issue of impingement with the introduction of an anti-impingement guide. Many large series have reported no revisions for wear in the absence of impingement.8-10,33,19,34
According to National Joint Registers, component loosening is one of the most common causes of failure, although many clinical studies report much lower rates. Late loosening has been attributed to the accumulated effects of impact loading from impingement of the front of the bearing on the femoral condyle when the knee is in full extension.12
Only one of the 213 knees (0.5%) implanted underwent dislocation of the bearing: this accords with the larger Oxford studies, namely Pandit et al8 (0.6%), Price and Svärd16 (1%) and Yoshida et al34 (0.8%).
The ten-year survivorship, including all revisions as an end point, was 88%. When revisions unrelated to the implant are eliminated, the ten-year survivorship was 95%, proving that the design of the implant itself is successful in retaining function and fixation in the long term. The option of retaining the medial implant and resurfacing the lateral compartment offers a less invasive, simpler solution for the knee with uncomplicated progression of osteoarthritis in the lateral compartment.
This series also shows how recurrent haemarthrosis can result in revision (three knees in this series), as such bleeding needs to be stopped before it causes a generalised arthrosis. The frequent prescribing of anti-platelet therapy may play a role in haemarthrosis of the knee.
The designer series reported a ten-year survivorship of 96%.8 Independent centres have reported ten-year survivorship of 95%34 and 94%.7 The 12th annual report of the United Kingdom National Joint Registry reports the ten-year survivorship of the Oxford UKA at 88%.35 Compared with the various studies mentioned above, our sample size was much smaller. This may explain our slightly lower survivorship on the basis of surgical caseload in determining the survival of UKAs.36
The strengths of this study are its prospective collection of data in a practice-based registry, and the long-term follow-up, although it is still a retrospective (longitudinal cohort) study which comes with its own limitations. A weakness of the study is the 30 patients lost to follow-up in the first year: this adversely affects the survivorship figures.
In conclusion, this is the first ten-year follow-up of the Oxford mobile-bearing medial UKA undertaken in the United States, and showed good survivorship and excellent function in a wide selection of patients with AMOA and AVN, without excluding patients on the grounds of age or BMI.
Take home message: Medial unicompartmental knee arthroplasty with the Oxford knee have proven good long-term survivorship and functionality in patients with osteoarthritis, without excluding for age or BMI.
1 White SH , LudkowskiPF, GoodfellowJW. Anteromedial osteoarthritis of the knee. J Bone Joint Surg [Br]1991;73-B:582–586. Google Scholar
2 Emerson RH Jr , AyersC, HeadWC, HigginsLL. Surgical closing in primary total knee arthroplasties: flexion versus extension. Clin Orthop Relat Res1996;331:74–80.CrossrefPubMed Google Scholar
3 Insall JN , DorrLD, ScottRD, ScottWN. Rationale of the Knee Society clinical rating system. Clin Orthop Relat Res1989;248:13–14.PubMed Google Scholar
4 Kozinn SC , ScottR. Unicondylar Knee Arthroplasty. J Bone Joint Surg [Br]1989;71-B:145–150.PubMed Google Scholar
5 Murray DW , CarrAJ, BulstrodeC. Survival analysis of joint replacements. J Bone Joint Surg [Br]1993;75-B:697–704.PubMed Google Scholar
6 Peto R , PikeMC, ArmitageP, et al.Design and analysis of randomized clinical trials requiring prolonged observation of each patient. II. analysis and examples. Br J Cancer1977;35:1–39.CrossrefPubMed Google Scholar
7 Price AJ , DoddCA, SvärdUG, MurrayDW. Oxford medial unicompartmental knee arthroplasty in patients younger and older than 60 years of age. J Bone Joint Surg [Br]2005;87-B:1488–1492.CrossrefPubMed Google Scholar
8 Pandit H , JenkinsC, GillHS, et al.Minimally invasive Oxford phase 3 unicompartmental knee replacement: results of 1000 cases. J Bone Joint Surg [Br]2011;93-B:198–204.CrossrefPubMed Google Scholar
9 Kort NP , van RaayJJ, CheungJ, JolinkC, DeutmanR. Analysis of Oxford medial unicompartmental knee replacement using the minimally invasive technique in patients aged 60 and above: an independent prospective series. Knee Surg Sports Traumatol Arthrosc2007;15:1331–1334.CrossrefPubMed Google Scholar
10 Rajasekhar C , DasS, SmithA. Unicompartmental knee arthroplasty. 2- to 12-year results in a community hospital. J Bone Joint Surg [Br]2004;86-B:983–985.CrossrefPubMed Google Scholar
11 Kim KT , LeeS, KimJH, et al.The Survivorship and Clinical Results of Minimally Invasive Unicompartmental Knee Arthroplasty at 10-Year Follow-up. Clin Orthop Surg2015;7:199–206.CrossrefPubMed Google Scholar
12 Heller S , FenichelI, SalaiM, LuriaT, VelkesS. The Oxford unicompartmental knee prosthesis for the treatment of medial compartment knee disease: 2 to 5 year follow-up. Isr Med Assoc J2009;11:266–268.PubMed Google Scholar
13 Kristensen PW , HolmHA, VarnumC. Up to 10-year follow-up of the Oxford medial partial knee arthroplasty--695 cases from a single institution. J Arthroplasty2013;28(Suppl):195–198.CrossrefPubMed Google Scholar
14 Murray DW , PanditH, Weston-SimonsJS, et al.Does body mass index affect the outcome of unicompartmental knee replacement?Knee2013;20:461–465.CrossrefPubMed Google Scholar
15 Mercier N , WimseyS, SaragagliaD. Long-term clinical results of the Oxford medial unicompartmental knee arthroplasty. Int Orthop2010;34:1137–1143.CrossrefPubMed Google Scholar
16 Price AJ , SvärdU. A second decade lifetable survival analysis of the Oxford unicompartmental knee arthroplasty. Clin Orthop Relat Res2011;469:174–179.CrossrefPubMed Google Scholar
17 Pandit H , MancusoF, JenkinsC, et al.Lateral unicompartmental knee replacement for the treatment of arthritis progression after medial unicompartmental replacement. Knee Surg Sports Traumatol Arthrosc2016 March. (Epub ahead of print)CrossrefPubMed Google Scholar
18 Goodfellow J , O’ConnorJ. The mechanics of the knee and prosthesis design. J Bone Joint Surg [Br]1978;60-B:358–369.CrossrefPubMed Google Scholar
19 Svärd UC , PriceAJ. Oxford medial unicompartmental knee arthroplasty. A survival analysis of an independent series. J Bone Joint Surg [Br]2001;83-B:191–194.CrossrefPubMed Google Scholar
20 Lombardi AV Jr , BerendKR, WalterCA, Aziz-JacoboJ, CheneyNA. Is recovery faster for mobile-bearing unicompartmental than total knee arthroplasty?Clin Orthop Relat Res2009;467:1450–1457.CrossrefPubMed Google Scholar
21 Dervin GF , CarruthersC, FeibelRJ, et al.Initial Experience With the Oxford Unicompartmental Knee Arthroplasty. J Arthroplasty2011;26:192–197.CrossrefPubMed Google Scholar
22 Pandit H , HamiltonTW, JenkinsC, et al.The clinical outcome of minimally invasive Phase 3 Oxford unicompartmental knee arthroplasty: a 15-year follow-up of 1000 UKAs. Bone Joint J2015;97-B:1493–1500.CrossrefPubMed Google Scholar
23 Hurst JM , BerendKR, AdamsJB, LombardiAV Jr. Radiographic comparison of mobile-bearing partial knee single-peg versus twin-peg design. J Arthroplasty2015;30:475–478.CrossrefPubMed Google Scholar
24 Kapetanos GA , PapavasiliouKA, MakrisV, et al.Recurrent spontaneous hemarthrosis after total knee arthroplasty successfully treated with synoviorthesis. J Arthroplasty2008;23:931–933.CrossrefPubMed Google Scholar
25 Zermatten P , MunzingerU. The Oxford II medial unicompartmental knee arthroplasty: an independent 10-year survival study. Acta Orthop Belg2012;78:203–209.PubMed Google Scholar
26 Asanuma K , ItoH, OgawaA, et al.Recurrent hemarthrosis after unicompartmental knee arthroplasty. Orthopedics2011;34:578–580.CrossrefPubMed Google Scholar
27 Kawata M , InuiH, TaketomiS, et al.Recurrent hemarthrosis after total knee arthroplasty caused by the impingement of a remnant lateral meniscus: a case report. Knee2014;21:617–619.CrossrefPubMed Google Scholar
28 Rukavina A , KerkhoffsGM, SchneiderP, KusterMS. Recurrent hemarthrosis after total knee arthroplasty. Knee Surg Sports Traumatol Arthrosc2010;18:898–900.CrossrefPubMed Google Scholar
29 Takezawa Y , AraiY, FujitaS, et al.A case of selective arterial embolization for recurrent hemarthrosis after total knee arthroplasty. J Orthop Sci2013;18:679–682.CrossrefPubMed Google Scholar
30 Valentino LA . Blood-induced joint disease: the pathophysiology of hemophilic arthropathy. J Thromb Haemost2010;8:1895–1902.CrossrefPubMed Google Scholar
31 Yamakado K , ArakawaH, HayashiS. Arthroscopic observation was useful to detect loosening of the femoral component of unicompartmental knee arthroplasty in a recurrent hemoarthrosis. Sports Med Arthrosc Rehabil Ther Technol2012;4:8.CrossrefPubMed Google Scholar
32 Kendrick BJ , LonginoD, PanditH, et al.Polyethylene wear in Oxford unicompartmental knee replacement: a retrieval study of 47 bearings. J Bone Joint Surg [Br]2010;92-B:367–373.CrossrefPubMed Google Scholar
33 Lim HC , BaeJH, SongSH, KimSJ. Oxford phase 3 unicompartmental knee replacement in Korean patients. J Bone Joint Surg [Br]2012;94-B:1071–1076.CrossrefPubMed Google Scholar
34 Yoshida K , TadaM, YoshidaH, et al.Oxford phase 3 unicompartmental knee arthroplasty in Japan--clinical results in greater than one thousand cases over ten years. J Arthroplasty2013;28(Suppl):168–171.CrossrefPubMed Google Scholar
35 No authors listed. National Joint Registry 12th Annual Report. http://www.njrcentre.org.uk/njrcentre/Portals/0/Documents/England/Reports/12th%20annual%20report/NJR%20Online%20Annual%20Report%202015.pdf (date last accessed 30 June 2016). Google Scholar
36 Liddle AD , PanditH, JudgeA, MurrayDW. Effect of Surgical Caseload on Revision Rate Following Total and Unicompartmental Knee Replacement. J Bone Joint Surg [Am]2016;98:1–8.CrossrefPubMed Google Scholar
Author contributions:
R. H. Emerson: Senior author and senior surgeon, Performed all surgeries on patients in this study, Final edit of manuscript.
O. Alnachoukati: Primary and corresponding author, Performed statistical analysis on all data, Data capture, acquisition and compilation, Patient outreach.
J. Barrington: Second edit and contribution to introduction and discussion sections.
K. Ennin: Third edit and contribution to introduction and discussion sections.
This is an open-access article distributed under the terms of the Creative Commons Attributions licence (CC-BY-NC), which permits unrestricted use, distribution, and reproduction in any medium, but not for commercial gain, provided the original author and source are credited.
We would like to thank Texas Health Presbyterian Hospital of Plano for their support of this work.
Although none of the authors has received or will receive benefits for personal or professional use from a commercial party related directly or indirectly to the subject of this article, benefits have been or will be received but will be directed solely to a research fund, foundation, educational institution, or other non- profit organization with which one or more of the authors are associated.
This article was primary edited by A. C. Ross
