




Abstract
Aims
Europe has found itself at the epicentre of the COVID-19 pandemic. Naturally, this has placed added strain onto healthcare systems internationally. It was feared that the impact of the COVID-19 pandemic could overrun the Irish healthcare system. As such, the Irish government opted to introduce a national lockdown on the 27 March 2020 in an attempt to stem the flow of admissions to hospitals. Similar lockdowns in the UK and New Zealand have resulted in reduced emergency department presentations and trauma admissions. The aim of this study is to assess the effect of the national lockdown on trauma presentations to a model-3 hospital in Dublin, Ireland.
Methods
A retrospective study was conducted. All emergency department presentations between 27 March 2019 to 27 April 2020 and 27 March 2020 to 27 April 2020 were cross-referenced against the National Integrated Medical Imaging System-Picture Archiving Communication System (NIMIS-PACS) radiology system to identify those with radiologically proven skeletal trauma. These patients were grouped according to sex, age, discharge outcome, mechanism of injury, and injury location.
Results
A 21% decrease in radiologically proven trauma was observed on comparison with the same time-period last year. Additionally, a 40% reduction in trauma admissions was observed during the COVID-19 lockdown. A 60% reduction in sports-related injuries and road traffic accident-related injuries was noted during the national lockdown. However, a 17% increase was observed in patients sustaining trauma because of domestic accidents.
Conclusion
Variation was observed in both the volume and nature of trauma presentations during the COVID-19 lockdown. As would be expected, a reduction was seen in the number of injuries resulting from outdoor activities. Interestingly, increased rates of domestic injuries were seen during this period which could represent an unintended consequence of the prolonged period of lockdown.
Cite this article: Bone Joint Open 2020;1-6:261–266.
Introduction
While the origins of the severe acute respiratory syndrome coronavirus-2 (SARS-CoV-2) and the resultant coronavirus disease 2019 (COVID-19) are found in China’s Hubei province it is unique among modern pandemics in that its epicentre has come to be in Europe.1 Previous pandemics such as the Spanish Flu (H1N1), SARs (SARS-CoV-1), Middle East Respiratory Syndrome Coronavirus (MERS-CoV), and Ebola Virus (EBV) have predominantly affected America, Asia, the Middle-East, and Africa respectively.
At the time of writing, 137,047 COVID-19-related deaths have occurred in Europe, representing 57% of the global mortality rate.2 As such, COVID-19 represents a new and unique challenge to healthcare systems worldwide, but potentially mostly so in Europe.
In Ireland, COVID-19 has placed additional strain on an already stretched healthcare system. If left unchecked, it was feared that COVID-19 had the potential to overwhelm the health service. For this reason the Irish government opted to implement a host of restrictive measures aimed at curtailing the spread of the disease.
On 27 March 2020, the Irish government commenced a national lockdown in an attempt to “flatten the curve”. Non-essential services were shutdown, with widespread travel restrictions, closure of public spaces, and cancellation of sporting events.3 These restrictive measures have affected the day-to-day living of every citizen in the country, and the resultant behavioural changes have never before been witnessed in the history of the state.
Nevertheless, trauma is an inevitability and the COVID-19 pandemic has had a complex impact on the delivery of trauma care worldwide. In the UK, the British Orthopaedic Association (BOA) have released guidelines pertaining to the management of acute trauma during these unprecedented times. Similarly, the Royal College of Surgeons Ireland (RCSI) have acknowledged the potential impact of the COVID-19 crisis in Ireland and have released recommendations for the delivery of trauma services.4
Internationally, anecdotal evidence from Italy and research from New Zealand and the UK have reported a significant decrease in the number of trauma cases presenting during the COVID-19 lockdown.5-7 However, no research exists examining the impact of the national lockdown on the Irish cohort.
As such, the aim of this study is to quantify the impact of the national lockdown on trauma presentations to a model-3 hospital in Ireland. It is hoped that this research may provide an indication of the temporal change in acute trauma care during the COVID-19 lockdown and as such assist in allowing appropriate allocation of resources during these unprecedented times.
Methods
A retrospective study was conducted in Connolly Hospital, which is located in the Dublin west suburb of Blanchardstown. Connolly Hospital is a model-3 hospital, which provides emergency medical services to the north Dublin catchment area with an estimated population of 331,000 people.8
Data was collected using the hospital’s electronic patient database. All patients presenting to the emergency department during the one-month period from 27 March 2020 to 27 April 2020 and from 27 March 2019 to 27 April 2019 were identified retrospectively from a prospectively collected database. Patient IDs were cross-referenced against the National Integrated Medical Imaging System-Picture Archiving Communication System (NIMIS-PACS) radiology platform to identify patients with radiologically proven fractures. The mechanisms of injury and locations of injury were documented in emergency department notes, imaging requests, or as part of routine outpatient follow-up post-injury.
Data was compiled, anonymized, and analyzed using Excel (Microsoft, Redmond, Washington, USA) on a password-protected departmental computer. Descriptive statistics were calculated for all desired variables. Associations between patients characteristics, treatment outcome, mechanisms of injury, and locations of injury were then examined in bivariate analysis using χ2 tests. Ethical approval was granted by the hospitals Research Ethics Board (REC).
Results
Trauma presentations
The findings of this study can be seen in Table I. A significant reduction was observed in trauma rates during the lockdown period. 136 patients presented to ED with radiologically proven skeletal trauma during the study period in comparison with 174 patients during the same period in 2019, representing a 22% in trauma rates (χ2 (1, N = 310) = 4.66, p = 0.03).
Table I.
Comparison of trauma presentations from 27 March 2019 to 27 April 2019 versus 27 March 2020 to 27 April 2020.
| 2019 | 2020 | |||||
|---|---|---|---|---|---|---|
| n | % | n | % | % change | p-value* | |
| Overall | 174 | 136 | -21% | 0.031 | ||
| Sex | ||||||
| Male | 96 | 55% | 62 | 46% | -35% | < 0.001 |
| Female | 77 | 45% | 74 | 54% | -4% | |
| Age bands | ||||||
| 16 to 64 | 120 | 69% | 83 | 61% | -31% | < 0.001 |
| > 65 | 54 | 31% | 53 | 39% | -2% | |
| Median age | 44 | 55 | ||||
| Mean age | 49 | 54 | ||||
| Treatment outcome | ||||||
| Admitted | 66 | 38% | 39 | 29% | -40% | 0.002 |
| Discharged | 6 | 4% | 4 | 3% | -33% | |
| Outpatient follow-up | 101 | 58% | 93 | 68% | -8% | |
| Mechanism of injury | ||||||
| Mechanical fall | 61 | 35% | 62 | 46% | + 2% | |
| Sports | 39 | 22% | 15 | 11% | -62% | 0.001 |
| Blunt trauma | 10 | 6% | 8 | 6% | -20% | |
| Road traffic accident | 10 | 6% | 4 | 3% | -60% | |
| Pedestrian | 9 | 5% | 9 | 7% | N/a | |
| Crush injury | 8 | 5% | 4 | 3% | -50% | |
| Unknown | 8 | 5% | 3 | 2% | -63% | |
| Inversion injury | 7 | 4% | 5 | 4% | -29% | |
| Assault | 7 | 4% | 4 | 3% | -43% | |
| Fall down stairs | 5 | 3% | 11 | 8% | + 55% | |
| Other | 7 | 4% | 1 | < 1% | -86% | |
| Fall from height > 2 m | 3 | 1% | 10 | 7% | + 70% | 0.003 |
| Location of injury | ||||||
| Home | 67 | 39% | 81 | 60% | + 17% | |
| Public road | 34 | 20% | 25 | 18% | -26% | |
| Public space | 33 | 19% | 8 | 6% | -76% | 0.001 |
| Unknown | 14 | 8% | 3 | 2% | -79% | |
| Workplace | 11 | 6% | 9 | 7% | -18% | |
| Nursing home | 8 | 5% | 8 | 6% | N/a | |
| Public building | 6 | 3% | 1 | < 1% | -83% | |
| Other | 1 | < 1% | 1 | < 1% | N/a |
-
*
p-values derived from χ2 tests for independence, p < 0.05 deemed significant.
During the COVID-19 lockdown, 39 patients required inpatient admission for trauma management. In comparison, during the same period in 2019, 66 patients required hospital admission. This equated to an overall 40% reduction in hospital admission rates for trauma during the COVID-19 lockdown (χ2 (1, N = 105) = 6.94, p = .002).
Sex and age band
A significant reduction was observed in rates of musculoskeletal injury among males during the COVID-19 lockdown. Of the 2020 cohort, 46% (n = 62) were male, while 54% (n = 74) were female. In comparison, in 2019 the cohort was 55% (n = 96) male and 45% (n = 77) female, representing a 35% reduction in trauma among males (χ2 (1, N = 158) = 7.32, p = < 0.001).
During the COVID-19 lockdown, the mean age of patients was 54 years and the median age of the cohort was 55 years. The cohort from 2019 had an average age of 49 years, with a median age of 44 years. Irrespective of time period analyzed, the majority of trauma in the 16- 64-year-old age group occurred in males. Similarly, in patients aged 65 years or older, females were predominately affected, with no significant differences observed between groups.
In all, 61% (n = 83) of patients presenting during the COVID-19 lockdown were aged 16 to 64 years, while 39%(n = 53) of patients were aged 65 years or older. Similarly in 2019, 69% (n = 120) of patients were aged between 16 to 64 years, while 31% (n = 54) were aged 65 years or over.
Mechanism of injury
Variations in the mechanism of injury are outlined in Figure 1. Falls of less than two metres which were mechanical in nature were termed “mechanical falls” and this was the most common injurious mechanism across both time periods. During the COVID-19 lockdown, 46% (n = 62) of patients cited a mechanical fall as their mechanism of injury, followed by injuries from sports and recreation (11%, n = 15), falling down stairs (8%, n = 11), pedestrian injuries (7%, n = 9), blunt trauma (8%, n = 6), falls from ladders (7%, n = 5), inversion injuries (4%, n = 5), with crush injuries, road traffic accidents, and assaults cited as the injurious mechanism in 3% of cases.
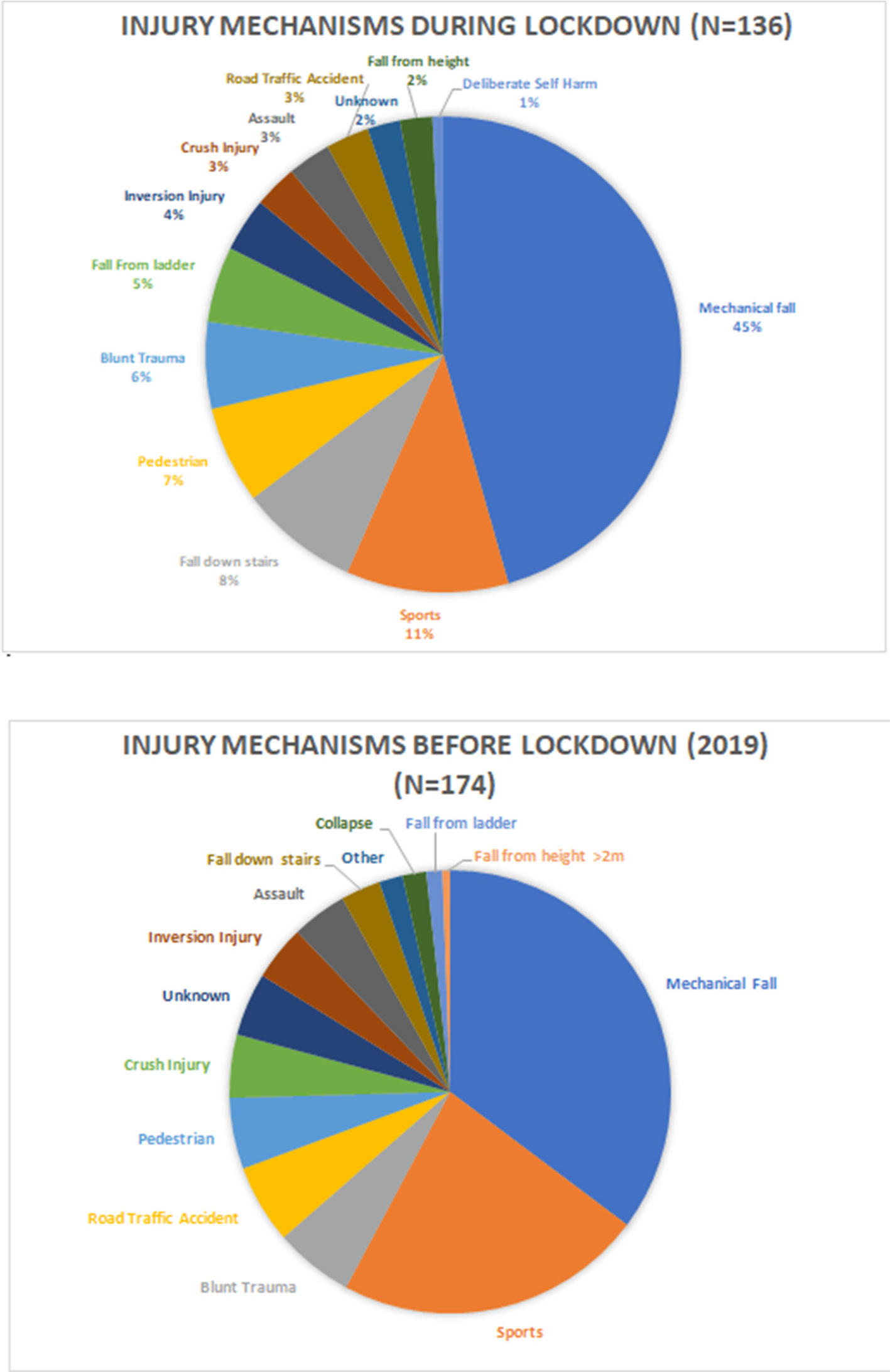
Fig. 1
Mechanisms of injury during COVID-19 lockdown versus before lockdown in 2019.
In comparison with the 2019 cohort, there was an approximately 60% reduction in patients sustaining injuries during both recreational and road traffic accidents during the COVID-19 lockdown. A similar reduction was seen in injuries resulting from assaults, approximately 43% however owing to the relatively low numbers observed in both groups, these results did not reach significance.
A significant reduction was seen in sports-related trauma during the COVID-19 lockdown in comparison with 2019 (χ2 (1, N = 54)= 10.66, p = 0.001).
Interestingly, a 70% increase was noted in patients presenting with trauma as a result of falls from height during the COVID-19 lockdown, specifically, reports of falls from ladders at home increased threefold. However, these results were deemed non-significant, owing to the low-numbers. These findings are outlined in Figure 2.
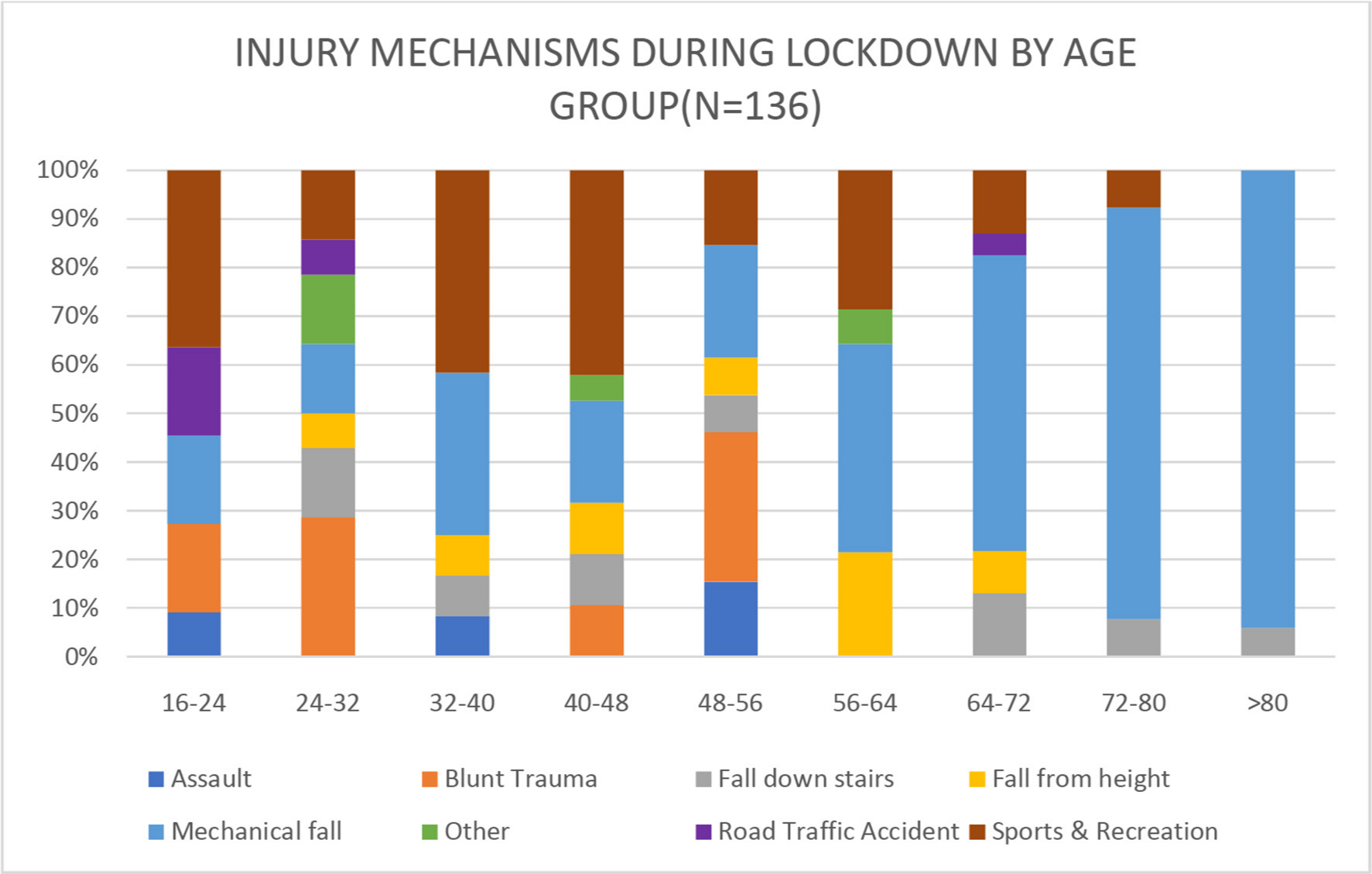
Fig. 2
Injury mechanisms during lockdown by age group.
Place of Injury
Home was the most common location of injury across both cohorts; however, large variation was seen between the two time periods. In all, 60% (n = 81) of patients cited home as the site of injury during the COVID-19 lockdown, while 39% (n = 67) sustained trauma at home during the same period in 2019.
A significant reduction was observed in patients sustaining injuries in public spaces during the COVID-19 lockdown (χ2 (1, N = 41)= 14.05, p = < 0.001). A reduction in volume of injury was seen across all other locations analysed, excluding nursing homes which was the location of injury for eight patients in both groups.
Discussion
On 27 March 2020, the Irish government commenced a national lockdown in an attempt to “flatten the curve” of COVID-19 spread. While the goal of this lockdown was to curtail the spread of this deadly pandemic it appears to have had knock on effects on the incidence of traumatic injuries in Ireland.
On comparison of our patient cohort with that of the Irish Major Trauma Audit (MTA) in 2016 our patient group appear grossly comparable to the national average.9 The mean age of patients identified by the MTA was 55 years, while that of our cohort was 54. Similarly, the MTA concluded that the predominance of injuries suffered in patients aged 0 to 54 years were male, with females being the predominant sex injured in those aged 54 years or older.9 These findings were replicated in our study.
The aim of our study was to assess for variation in the number and manner of trauma presentations to our hospital during the COVID-19 national lockdown. Our study found that fewer patients presented with radiological proven skeletal trauma during the lockdown, and of those patients who presented with trauma, fewer required hospital admission.
Variation was seen in the mechanism of injury when comparison was made with data from 2019. As would be expected a significant reduction in injuries from sports and recreation was observed during the lockdown (χ2 (1, N = 54) = 10.66, p = 0.001). A marked reduction in road traffic accidents was also observed, with smaller reductions also seen in injuries resulting from assaults. The majority of differences observed in mechanisms of injury failed to reach statistical significance, which is likely due to the relatively small sample size.
Variation was also observed in the location of injury during the national lockdown. A large increase was seen in patients sustaining injuries at home. Domestic injuries were most commonly due to mechanical falls, falls down stairs, and falls from ladders.
While there is a relative dearth of research in this field, the results of this study are paralleled in research conducted in both the European and Australasian context. Thornton noted a 25% reduction in accident and emergency (A&E) department presentations during the first week after lockdown in the UK.6 The authors postulated that the reduction in A&E presentations was potentially due to the effect of social isolation and lower vehicle use during lockdown.6
The effect of national lockdown on trauma in New Zealand was reported by Christey et al,7 and their results are grossly comparable to this study. Authors noted a 43% reduction in trauma admissions during national lockdown in New Zealand. Similarly, a reduction in injuries sustained by males under the age of 65 years was observed.7 Furthermore, the authors observed a reduction in both sports-related injuries and road traffic accident-related injuries.7 As with our study, mechanical falls represented the most common cause of trauma, most frequently occurring in the over 65 years age group.7
The findings of this study have important public health implications. While instituting a national lockdown has predictably led to a decrease in trauma among the more mobile under 65 years population, trauma rates among the elderly remain unchanged and rates of domestic injuries have increased. The home is the still the most common site of injury and falls from a less than two metres in height are the most common injurious mechanism. The need for a public health initiative to reduce the risk of falls at home has been acknowledged by the Irish government. The AFFINITY National Falls and Bone Health Project was commenced in December 2019.10 Particular emphasis should be placed on public health initiatives like this during the coming months. These initiatives increase awareness of the preventable nature of falls, and aim to reduce the rate of falls among the elderly. A reduction in falls among the elderly in the coming months would contribute greatly in reducing the strain on our health system as a whole during the COVID-19 crisis.10
In the UK, a dedicated public health initiate has been launched by the Royal Society for the Prevention of Accidents (ROSPA) to decrease the rates of domestic injuries during the COVID-19 crisis, and to reduce rates of domestic injuries on a national leve.11
Furthermore, consideration should be given to the need for a public health initiative highlighting the potential dangers of do-it-yourself (DIY) activities during the national lockdown. A large increase in purchasing of DIY products such as paint, ladders, and gardening tools was reported in the lead up to the lockdown.12 This coincides with a marked increase in falls from a height during the lockdown, specifically falls from a ladder. Governments should consider issuing specific warnings to highlight the potential dangers of DIY activities during lockdown, particularly highlighting ladder safety.
This study also has important implications for resource allocation and consolidation of trauma care services in Ireland. We observed a 40% reduction in trauma admissions during the study period. A decrease in trauma admissions reflects decreased demand on trauma services during the national lockdown. This could feasibly allow temporary redeployment of some orthopaedic doctors to areas of higher demand during this global pandemic should the need arise.
Conclusion
The restrictions imposed on Irish citizens as a result of the national lockdown have had profound effects on the day-to-day life of the entire population. Naturally, as a result of stringent travel restrictions and advice for elderly individuals to “cocoon” fewer traumas are occurring outside of the home. However, trauma is an inevitability and a large increase in home-based injuries were seen in our cohort, specifically occurring as a result of mechanical falls, falling down stairs, and falls from ladders.
This study has some obvious limitations, we chose to only include patients presenting with fractures. Additionally, assumptions regarding trends of injury pattern with regards to location and mechanism should be interpreted with caution in some instances owing to the relatively low numbers of patients. Future studies would ideally identify all patients with musculoskeletal trauma and classify them according to injury severity, likely over a more prolonged period to identify a larger patient cohort.
However, this study contributes data to a field in which there is dearth of evidence at present. While similar results have been seen in New Zealand and the UK this is the only paper in the literature reporting the impact of national lockdown on the Irish cohort.6,7 As such, this paper could have important implications at both a local and national level, and allow for appropriate division of resources and planning of trauma services over the coming months and into the future if further lockdowns are required.
References
1. Ciotti M , Angeletti S , Minieri M , et al. COVID-19 outbreak: an overview . Chemotherapy . 2020 : 1 – 9 . Crossref PubMed Google Scholar
2. Control, E. C. f. D. P. a . COVID-19 situation update worldwide, as of 4 may 2020 , 2020 . Google Scholar
3. Department of Health, D. o. T . (ed Department of Taoiseach Department of Health) . 2020 . https://www.gov.ie/en/publication/cf9b0d-new-public-health-measures-effective-now-to-prevent-further-spread-o/ Google Scholar
4. Ireland, R. C. o. S . Trauma and orthopaedic surgery COVID-19 model of care . Ireland : Royal College of Surgeons , 2020 . Google Scholar
5. Fojut, R . 2020 . https://www.trauma-news.com/2020/03/how-coronavirus-is-affecting-trauma-systems-in-italy/ Google Scholar
6. Thornton J . Covid-19: A&E visits in England fall by 25% in week after lockdown . BMJ . 2020 ; 369 : m1401 . Google Scholar
7. Christey G , Amey J , Campbell A , Smith A . Variation in volumes and characteristics of trauma patients admitted to a level one trauma centre during national level 4 lockdown for COVID-19 in New Zealand . N Z Med J . 2020 ; 133 ( 1513 ): 81 – 88 . PubMed Google Scholar
8. Authority, H. I. a. Q . Health Information and Quality Authority . 2015 . https://www.hiqa.ie/system/files/inspectionreports/Report_Unannounced_Connolly Hospital_0.pdf Google Scholar
9. (NOCA), N. O. o. C. A . National Office of Clinical Audit . 2016 . https://www.noca.ie/documents/major-trauma-audit-national-report-2016 Google Scholar
10. Executive, H. S . (Ed department of health) (health service executive) . 2019 . https://www.hse.ie/eng/services/list/4/olderpeople/falls-prevention-and-bone-health/affinity-national-falls-and-bone-health-project-december-2019-update.pdf Google Scholar
11. Service, N. H . (ed Royal Society for the Prevention of Accidents) . 2020 . https://www.rospa.com/Campaigns-Fundraising/Current/Coronavirus Google Scholar
12. Wilson J . in The Irish Times . 2020 . https://www.irishtimes.com/news/ireland/irish-news/diy-stores-booming-as-people-keep-calm-and-carry-on-painting-1.4209158 Google Scholar
Author contributions
S. Fahy: Primary author, Collected the data, Undertook analysis, interpretation, and publication.
J. Moore: Collected the data, Undertook analysis.
M. Kelly: Collected the data, Undertook analysis.
O. Flannery: Collected the data, Undertook analysis and formatting.
P. Kenny: Senior author, Research supervisor, Designed the study.
Funding statement
This research received no specific grant from any funding agency in the public, commercial or not-for-profit sectors.
Ethical review statement:
Research discussed and approved by local Research Ethics Committee (REC).
© 2020 Author(s) et al. This is an open-access article distributed under the terms of the Creative Commons Attributions licence (CC-BY-NC-ND), which permits unrestricted use, distribution, and reproduction in any medium, but not for commercial gain, provided the original author and source are credited.
