




Abstract
Aims
We aim to objectively assess the impact of COVID-19 on mean total operative cases for all indicative procedures (as outlined by the Joint Committee on Surgical Training (JCST)) experienced by orthopaedic trainees in the deanery of the Republic of Ireland. Subjective experiences were reported for each trainee using questionnaires.
Methods
During the first four weeks of the nationwide lockdown due to COVID-19, the objective impact of the pandemic on each trainee’s surgical caseload exposure was assessed using data from individual trainee logbook profiles in the deanery of the Republic of Ireland. Independent predictor variables included the trainee grade (ST 3 to 8), the individual trainee, the unit that the logbook was reported from, and the year in which the logbook was recorded. We used the analysis of variance (ANOVA) test to assess for any statistically significant predictor variables. The subjective experience of each trainee was captured using an electronic questionnaire.
Results
The mean number of total procedures per trainee over four weeks was 36.8 (7 to 99; standard deviation (SD) 19.67) in 2018, 40.6 (6 to 81; SD 17.90) in 2019, and 18.3 (3 to 65; SD 11.70) during the pandemic of 2020 (p = 0.043). Significant reductions were noted for all elective indicative procedures, including arthroplasty (p = 0.019), osteotomy (p = 0.045), nerve decompression (p = 0.024) and arthroscopy (p = 0.024). In contrast, none of the nine indicative procedures for trauma were reduced. There was a significant inter-unit difference in the mean number of total cases (p = 0.029) and indicative cases (p = 0.0005) per trainee. We noted that 7.69% (n = 3) of trainees contracted COVID-19.
Conclusion
During the COVID-19 pandemic, the mean number of operative cases per trainee has been significantly reduced for four of the 13 indicative procedures, as outlined by the JCST. Reassignment of trainees to high-volume institutions in the future may be a plausible approach to mitigate significant training deficits in those trainees worst impacted by the reduction in operative exposure.
Take home message
The COVID-19 pandemic has significantly reduced the number of elective indicative procedures performed per orthopaedic trainee on a national level.
Introduction
Our understanding of what it means to be an orthopaedic surgeon has been challenged in recent times. The SARS-CoV-2 (COVID-19) pandemic has impacted on every facet of our humanity, most specifically on our role as surgeons, doctors, teachers, and family members.1 Orthopaedic trainees in particular have had to accommodate some colossal upheavals in the trajectory of their surgical training. Issues ranging from reduced/ceased operative exposure, professional examination and course cancellation, and the impact on prospective fellowship opportunities have caused considerable concern and upset to current orthopaedic surgeons in training.2 Many articles have acknowledged the unprecedented impact that this pandemic will have on trainees through the restructuring of residency programmes and the significant reduction in exposure to elective orthopaedic cases in particular.3 At no point in the literature, however, has the objective impact of the pandemic been assessed in relation to the reduction of surgical procedures performed by individual trainees. We aim to objectively assess the reduction in total operative cases (including all indicative procedures as outlined by the Joint Committee on Surgical Training (JCST)) experienced by orthopaedic trainees in the deanery of the Republic of Ireland through the analysis of surgical logbooks. Subjective experiences were also reported for each trainee in the deanery through the use of anonymous questionnaires.
Methods
We conducted an analysis of the objective and subjective orthopaedic trainee experience during the first four weeks of the nationwide lockdown due to COVID-19.
Objective training assessment
The objective impact of the pandemic on each trainee’s surgical exposure was assessed using data from individual logbook profiles submitted by each trainee in the deanery of the Republic of Ireland. Each trainee submitted their logbook detailing their caseload between 27 March 2020 and 27 April 2020. Each trainee also submitted logbooks for this same date range in 2019 and 2018. The latter two logbooks served as a control for comparative analyses.
The JCST has published guidelines detailing a minimum requirement of “indicative procedures” that must be performed by each orthopaedic trainee before certification of training can be confirmed.4 There are 13 of these indicative procedures. As well as the indicative procedures, each trainee must participate in 1,800 total procedures during their training and must be the primary operator for 70% (n = 1,260) of these.1 We report on the total number of cases that the trainee was involved with, either as operator or assistant.
In order to capture the effect of the pandemic on these outcomes variables, we analyzed the following variables from each logbook submitted: ‘total procedures’, ‘total indicative procedures’, ‘total arthroplasty’, ‘total osteotomy’, ‘total nerve decompression’, ‘total arthroscopy’, ‘total dynamic hip screw (DHS)’, ‘total hemiarthroplasty’, ‘total external fixator’, ‘total tendon repair’, ‘total intramedullary (IM) nail’, ‘total plate’, ‘total tension band wire’, ‘total Kirschner wire (k-wire)’, ‘total supracondylar fixation’. Independent predictor variables included the trainee grade (ST 3 to 8), the individual trainee, the unit that the logbook was reported from and the year in which the logbook was recorded.
Statistical analysis
Logbooks were analyzed by procedure and by unit. For each procedure, boxplot graphs were used to illustrate the mean number of indicative cases performed by each trainee for 2018, 2019 and 2020. For each unit, simple line diagrams were used to illustrate the unit-specific total caseload for each trainee for the four-week period in 2018, 2019 and 2020. As we were analyzing categorical predictor variables and interval outcome variables, we used the analysis of variance (ANOVA) test to assess for any statistically significant predictor variables of the outcome measures listed above. A p-value of less than 0.05 was taken to be statistically significant and all statistical analysis was performed using Stata/IC 13.1 for Mac (64-bit Intel) (StataCorp, College Station, Texas, USA).
Subjective training experience
The subjective experience of each trainee was captured using an electronic questionnaire. A total of 33 questions covered five main areas of concern for each trainee:
-
The impact of COVID-19 on surgical training.
-
Adaptive educational resources.
-
The impact on FRCS examinations.
-
The impact on fellowships.
-
Individual COVID-19 contact and contraction.
All responses were anonymous. Simple descriptive statistics with bar charts and pie charts were used to illustrate all data collected from these trainee questionnaires.
Results
Objective training
A total of 40 orthopaedic trainees participated in the study. All trainees returned the three relevant logbooks and 38 returned the anonymized questionnaires.
When analyzing the services provided by each unit at the time of the nationwide lockdown, it was found that 70% (n = 28) provided adult trauma services, 72.5% (n = 29) provided adult elective services, 47.5% (n = 19) provided paediatric trauma services, and 32.5% (n = 13) provided paediatric elective services (Figure 1).
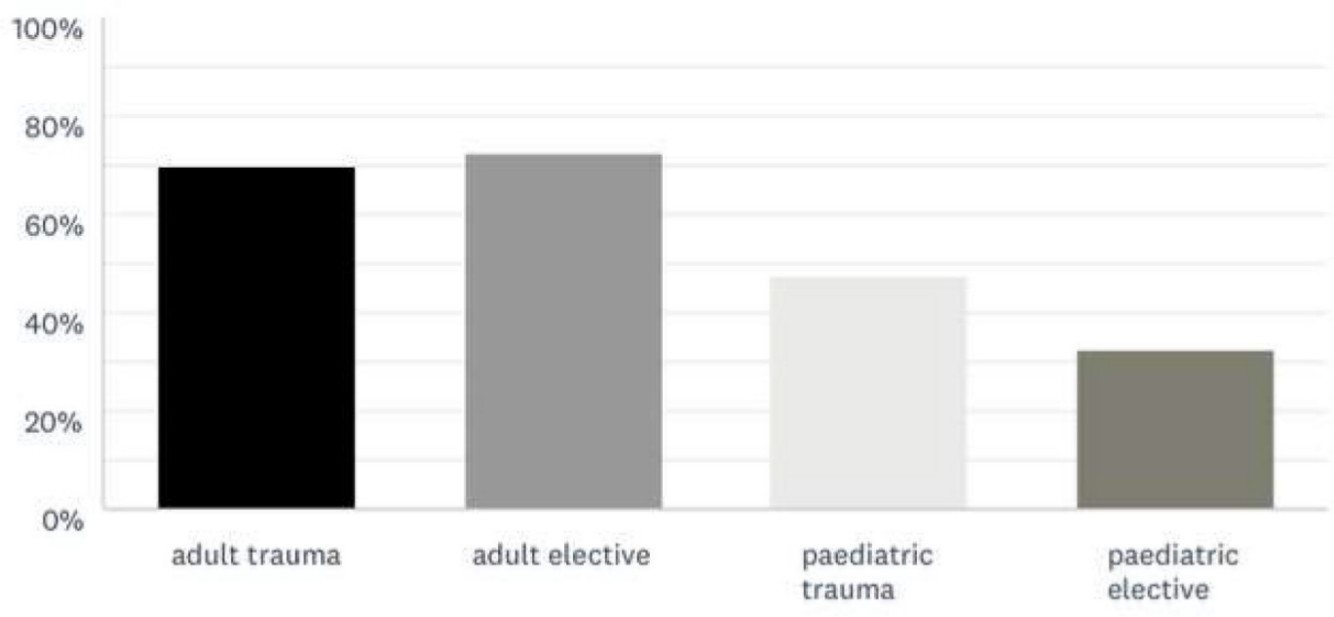
Fig. 1
Services provided in the unit of each trainee at the time of the nationwide lockdown.
The mean number of total procedures per trainee was 36.8 (7 to 99; standard deviation (SD) 19.67) in 2018, 40.6 (6 to 81; SD 17.90) in 2019 and 18.3 (3 to 65; SD 11.70) in the pandemic of 2020 (p = 0.043). The mean number of indicative procedures per trainee was 24.5 (1 to 74; SD 15.36) in 2018, 27.4 (1 to 66; SD 14.21) in 2019 and 12.4 (0 to 57; SD 10.16) in the pandemic of 2020 (p = 0.001). Figure 2 and Table I illustrate the breakdown across the three years of the mean number of indicative procedures per trainee. Of the four elective procedures included in the indicative list, all four were noted to have a significantly lower mean number of cases performed per trainee during the pandemic when compared to the same date range in 2018 and 2019. Significant reductions were noted for arthroplasty (p = 0.019), osteotomy (p = 0.045), nerve decompression (p = 0.024), and arthroscopy (p = 0.024).
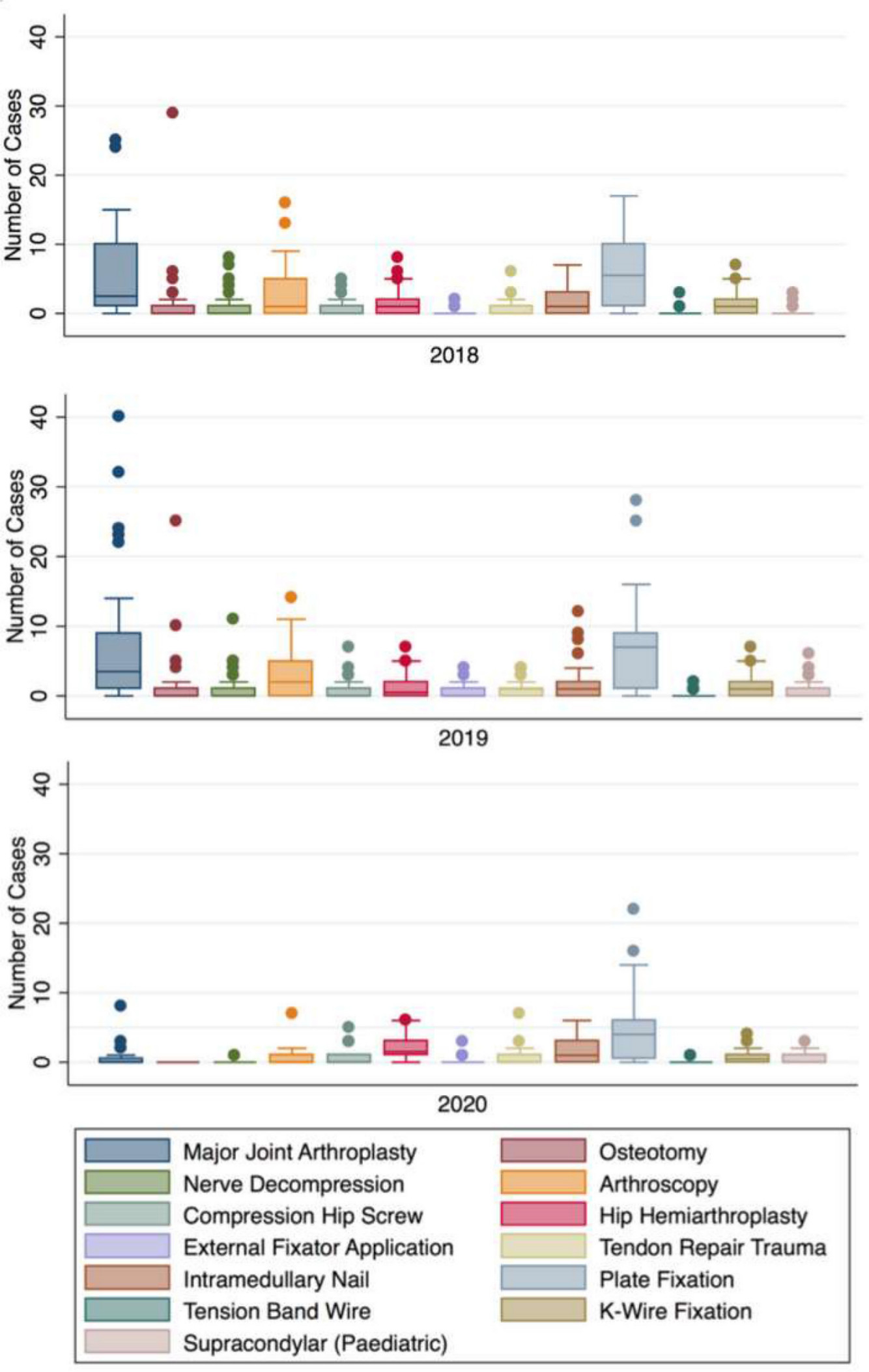
Fig. 2
Boxplots demonstrating the mean number of indicative procedures in 2018 (a), 2019 (b), and 2020 (c).
Table I.
The mean number of indicative procedures performed per trainee in 2018, 2019, and 2020.
| Year | Arthroplasty | Osteotomy | Nerve decompression | Arthroscopy | DHS | Hemiarthroplasty | External fixator | Tendon Repair | IM Nail | Plate | Tension Band Wire | K-wire | SC fixation |
| 2018 | 5.39 | 1.44 | 1.31 | 3.10 | 0.78 | 1.5 | 0.29 | 0.60 | 1.65 | 6.05 | 0.21 | 1.34 | 0.31 |
| 2019 | 7.16 | 1.40 | 1.11 | 3.39 | 0.78 | 1.14 | 0.52 | 0.81 | 1.78 | 6.92 | 0.23 | 1.35 | 0.81 |
| 2020 | 0.52 | 0 | 0.05 | 0.5 | 0.7 | 1.8 | 0.25 | 0.6 | 1.67 | 4.87 | 0.12 | 0.75 | 0.4 |
| p-value* | 0.019 | 0.045 | 0.024 | 0.024 | 0.682 | 0.269 | 0.351 | 0.767 | 0.971 | 0.662 | 0.669 | 0.544 | 0.881 |
-
*
Analysis of variance (ANOVA) test.
-
DHS, dynamic hip screw; IM, intramedullary; SC, supracondylar (paediatric).
In contrast, there were nine indicative procedures for trauma and none of these procedures underwent a significant reduction in volume in 2020 relative to 2018 and 2019. The mean number of hip hemiarthroplasty procedures performed actually increased during the pandemic period (1.8 in 2020 vs 1.14 in 2019, and 1.5 in 2018). The mean number of DHS procedures, tendon repairs, and IM nails performed were unchanged. All other indicative procedures for trauma showed a slight reduction in absolute figures compared to 2019, but these did not reach statistical significance (Figure 2).
The respective unit that each trainee was assigned to had a significant impact on the mean number of cases performed in the analyzed time period. The highest number of cases per trainee was logged in the National Orthopaedic Hospital. This hospital had converted from providing exclusively elective surgery to providing only ambulatory trauma for all acute hospitals in Dublin as the acute hospitals had all been seconded for COVID-19 care. This was followed by a level 1 trauma centre which was in turn closely followed by a high-volume trauma unit in the South East of the country. There was a significant inter-unit difference in the mean number of total cases per trainee (p = 0.029) and the mean number of indicative cases per trainee (p = 0.0005). All units experienced a sharp reduction in the overall volume of cases in 2020. Regarding ‘unit 14’, 2020 was the only year between 2018 and 2020 that trainees were assigned to that unit in an official capacity (Figure 3). Regarding ‘unit 12’, 2020 was the only year between 2018 and 2020 that no trainees were assigned to that unit. This is reflected in the lack of cases listed per trainee in Figure 3 during 2020 for ‘unit 12’.
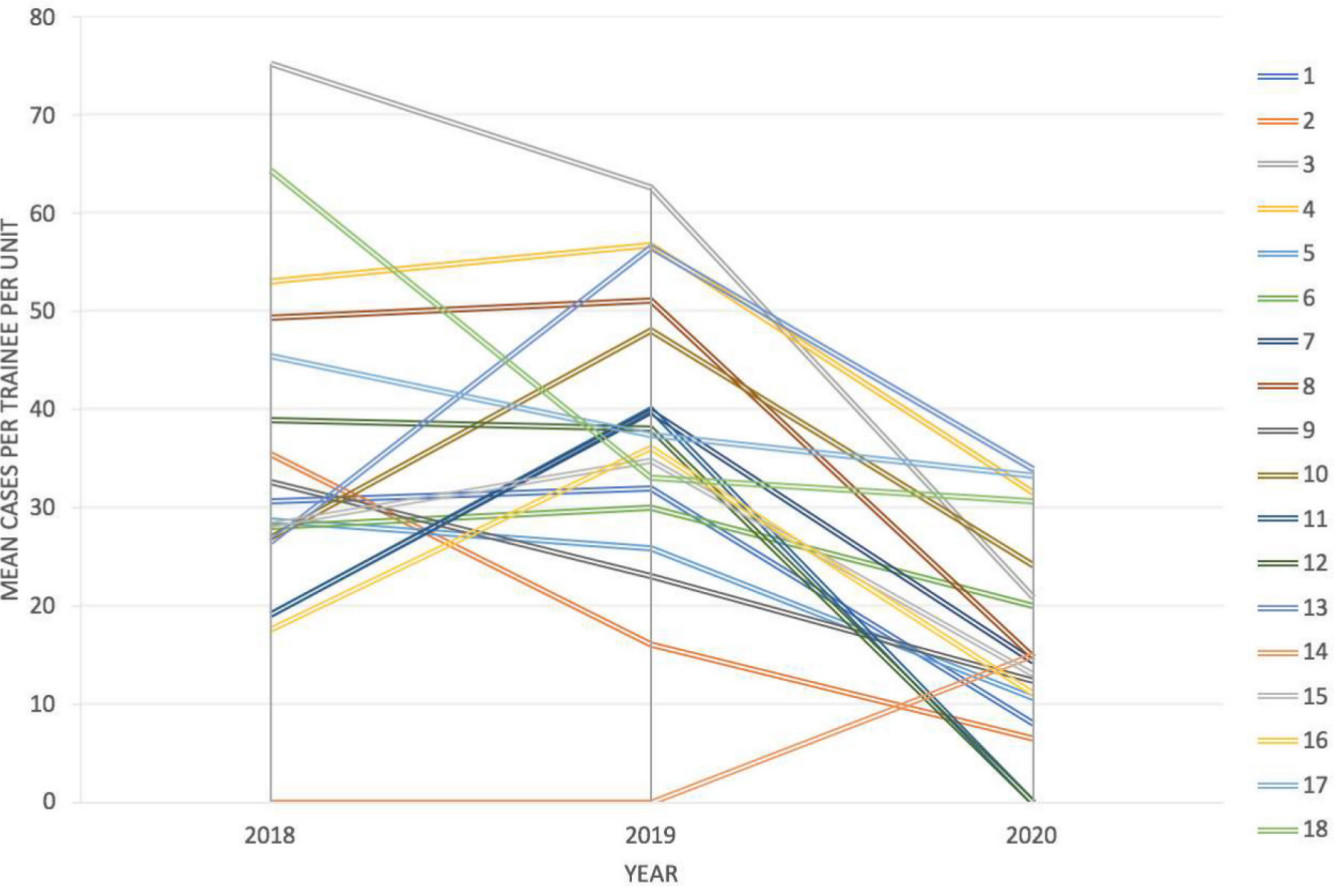
Fig. 3
The inter-unit breakdown of cases between 2018 and 2020. (No trainee in unit 12 for 2020; no trainee in unit 14 for 2018 and 2019).
The grade of the trainee did not have any significant impact on the mean number of total cases (p = 0.817) or the mean number of indicative cases (p = 0.211) performed in 2020 compared to 2018 and 2019. The individual trainee did not have any significant impact on the mean number of total cases (p = 0.742) or the mean number of indicative cases (p = 0.208) performed in 2020 compared to 2018 and 2019.
Subjective training experience
1. Impact of COVID-19 on surgical training
When asked about the perceived impact of COVID-19 on the trainee’s higher surgical training, over one-third (37.5%; n = 15) felt that the impact was negative (Figure 4).
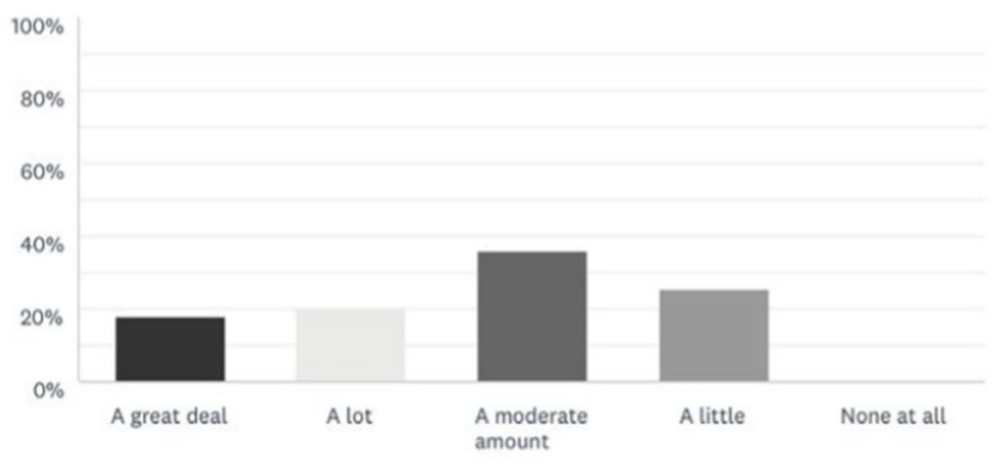
Fig. 4
“How negative has the impact of COVID-19 been on your higher surgical training in your opinion?”
In all, 90% (n = 36) of trainees felt that their logbook numbers had been significantly impacted and 35% (n = 14) were concerned to the degree that the felt they may require extended training in order to achieve certification. The majority of those concerned were in their earlier years of training. Of note, despite the reduction in surgical case load, all trainees were maintained in their role as an orthopaedic trainee and no trainee was seconded into a non-orthopaedic/medical/COVID-19-specific role.
2. Adaptive educational resources
With the introduction of a virtual core curriculum teaching platform by the Irish Institution of Trauma and Orthopaedic Surgery (IITOS), over 92% (n = 37) of trainees felt that this format either met or exceeded their expectations (Figure 5).
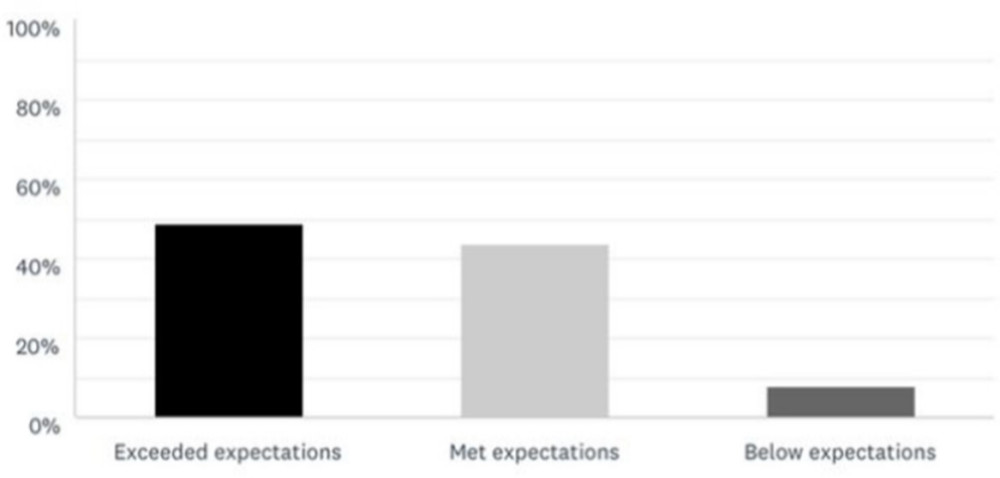
Fig. 5
“How do you rate the virtual core curriculum format?”
The commonest online resource utilized by all trainees was the Orthobullets website, followed by VuMedi, then by Arbeitsgemeinschaft für Osteosynthesefragen (AO) online educational materials.
3. Impact on FRCS examinations
Of all the 40 trainees, 82.5% (n = 33) were pre-FRCS examination status. Of these pre-FRCS trainees, 12 had been directly impacted by examination cancellation secondary to COVID-19. When asked how concerned they were about these cancellations, the majority of trainees that were impacted were either greatly concerned or very concerned (Figure 6).
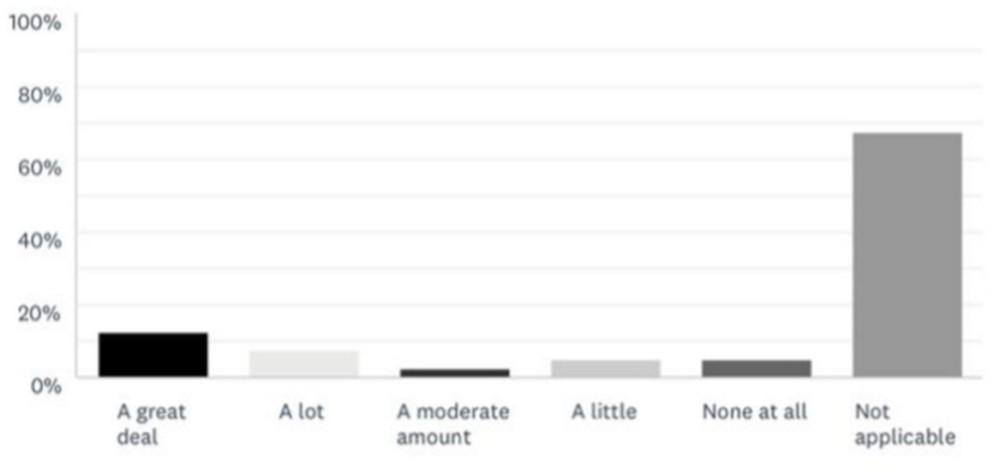
Fig. 6
“How concerned are you by the cancellation of the FRCS examinations?”
4. Impact on fellowships
Eight trainees were eligible for fellowship at the time of writing. For three of these, their plans for commencing fellowship were impacted negatively due to COVID-19. One was informed that the volume of elective surgery would be reduced. Another was told that they could not be guaranteed a place on the fellowship programme and the third trainee was told that the original start date would be delayed until further notice.
5. Individual COVID-19 contact and contraction
The final section of the questionnaire dealt with the personal health ramifications for each trainee due to COVID-19. After one month in lockdown, of the 38 trainees that responded to the question on COVID-contact, we reported that 21.05% (n = 8) had to undergo self-isolation, due to being COVID-contact positive, for two weeks under the instruction of the government and their local unit’s direction (Figure 7). Of the 39 trainees that responded to the question on COVID-19 contraction, 7.69% (n = 3) had to undergo self-isolation as a result of contracting the COVID-19 virus (Figure 8).
Fig. 7
Percentage of trainees (21.05%) that underwent self-isolation in the first month of lockdown due to being COVID-19-positive contact.
Fig. 8
Percentage of trainees (7.69%) that underwent self-isolation in the first month of lockdown due to being COVID-19-positive test.
Discussion
We identify the specific surgical procedures that underwent a reduction in volume for trainees as a result of the acute hospital response to the COVID-19 pandemic. As expected, all elective indicative procedures underwent a significant reduction in the mean number of cases per trainee during the four-week period assessed across the three years. Of the nine indicative procedures relating to trauma, only three showed an absolute reduction in the mean number of cases per trainee in 2020 (plate, tension band wire, k-wire). However, none of these showed a significant reduction in the mean number of cases per trainee. Of interest, the mean number of hemiarthroplasty cases per trainee actually increased to 1.8 in 2020 relative to 1.5 in 2018 and 1.14 in 2019. International reports have demonstrated a similar effect impacting more on elective services than trauma services.5 Quantifying the reduction in the mean number of indicative procedures per trainee during the pandemic will prove useful to inform decisions regarding trainees dealing with the expected yet unpredictable consequences of this pandemic.
This article describes the first objective figures reported to reveal the true extent of the impact of COVID-19 on the current orthopaedic trainee. This information is applicable to all deaneries under the guidance of the four Royal College of Surgeons in England, Edinburgh, Glasgow, and Ireland. All four colleges utilize the same indicative procedure metrics to assess the suitability of trainees for certification. For this reason we believe that these results will be of interest to the wider orthopaedic training community in the UK and Ireland.
In light of these significant reductions selecting for specific procedure types, 35% (n = 14) of trainees felt that they may need to extend their training in order to reach the appropriate competencies for certification. This anxiety among orthopaedic surgeons in training has been widely reported in the international literature with rates varying from 25% (n = 10) of trainees in Europe to 69% (n = 28) of trainees in the UK reporting that they may need additional training.6,7
This concern has led to the JCST issuing COVID-19 disruption training outcome guidelines. These take the form of added annual review of competence progression (ARCP) outcome categories, either directly (10.2) or indirectly (10.1), allowing for extra training if required as a consequence of a trainees inability to realise their full training potential in a post directly impacted as a result of COVID-19 restrictions.8 This makes appropriate allowances for trainees and their trainers during these challenging times. The opportunity also exists for trainees earlier in their training to compensate for a reduction in their numbers later on; however, those in the later years may not have this time and may now also have the added burden of a delayed FRCS examination to deal with.
Apart from the year in question, the only other predictor of the mean number of total cases per trainee (p = 0.029) and indicative cases per trainee (p = 0.0005) was the unit that the trainee was assigned to at the time of collating their logbooks. We identified the units that were most likely to be associated with a higher mean number of cases during the pandemic. Identification of the higher-volume units during the pandemic allows us to identify the more robust processes in place across the country. Many units have instigated a wide range of processes to cope with the change in trauma and elective service provision. Diversion of trainees, especially those with the greatest logbook deficits, into these high-volume units may be a viable option to equalize any discrepancy experienced by individual trainees secondary to the pandemic. Training bodies may need to consider flexibility and adjustment regarding trainee unit assignments in order to mitigate any undue impact on one trainee over another.
We know that reorganization of residency and fellowship programmes have become commonplace in training centres located in the epicentre of the pandemic in New York, USA, for example.9 We believe that similar attitudes will need to be adopted by governing bodies in the UK and Ireland also. We found that the individual trainee and their grade had no impact on the mean number of cases performed – implying that any discrepancies revealed in logbook numbers are truly systemic due to the pandemic and not based on the characteristics of any one individual trainee or their stage in training.
As well as documenting the negative impact of COVID-19, some positive aspects have also emerged. The use of a virtual platform to complete the mandatory teaching modules for all trainees has proved to be a great success, with over 92% of all trainees reporting that their expectations were either met or exceeded. In many ways, the pandemic has accelerated an inevitable paradigm shift toward a more accessible and convenient mode of orthopaedic education, albeit at the cost of social interaction among colleagues.10 Simulation, augmented reality, and distance learning are all weapons in the fight against COVID-19 for the modern orthopaedic trainee.11
Another positive aspect is in relation to the fellowship experience. We report on a number of trainees who will be impacted both in terms of case load and fellowship start dates. Despite these issues, we now know that greater “downtime” has allowed for a surge in academic engagement by trainees with a greater interest in collaborative academic efforts than were seen in the pre-COVID-19 era.12
Finally, and most important of all, is the physical and mental wellbeing of orthopaedic trainees across the world at this time. In as little as four weeks, over 20% (n = 8) of trainees had to self-isolate due to COVID-19 contact. In this same four-week period, over 7% (n = 3) of trainees actually contracted the virus, again requiring self-isolation in accordance with governmental guidelines. These figures will only increase as we progress deeper into the unknown territory of COVID-19. This isolation demonstrates a significant strain on each trainee personally, their family members, the hospital staffing levels and society as a whole. This dynamic is evident on an international scale where the interaction between trainees and COVID-19-positive patients is inevitable.3
Although we would not wish to renege on our privileged duty of providing care for all of our patients, it is imperative that we provide all forms of personal protective equipment (PPE) to those providing this care in these extremely high-risk environments. In certain studies, the provision of PPE has been suboptimal and dangerously inadequate.3 Creative new techniques and processes are being developed by the orthopaedic community in a conscious effort to preserve the vital resources that are needed at this time more than ever.13 As well as safeguarding the physical health of trainees, protecting the mental health of the entire surgical workforce is paramount during this prolonged period of adversity. As a community of surgeons, we must consider the likelihood of increased levels of burnout, stress and mental strain in the current trainee cohort as they move onward into the unknown post-COVID-19 era.14
Limitations
The experience of two trainees was exempt as they were undergoing out-of-programme training in 2020 and so were not assigned to a formal training post in the deanery of the Republic of Ireland. A further three trainees were not included on account of maternity leave, educational leave and a scheduled career break. Therefore, of a total 57 trainees, 52 were eligible for inclusion. Of these 52, 40 trainees volunteered their logbooks for analysis and 38 completed the questionnaire that was distributed. Although the final number of logbooks and questionnaires does not capture the entire trainee cohort from the deanery of the Republic of Ireland, the 40 trainees that did participate account for the vast majority of trainees and so our results do accurately reflect the experience of the average trainee in our deanery.
The mean number of operative cases was significantly reduced for four of the 13 indicative procedures, as outlined by the JCST, for orthopaedic trainees during the COVID-19 pandemic. All four procedures were elective in nature. Reassignment of trainees to high-volume institutions in future may be a plausible approach to mitigate significant training deficits in the trainees worst impacted by the reduction in operative case volume.
Orthopaedic trainees are at high risk of viral contraction and are likely to experience significant obstacles to their future career trajectory.
References
1. Graichen H . The role of an orthopaedic surgeon in the time of Covid-19 Pandemic-a German perspective . J Orthop . 2020 ; 19 : A1 – A3 . Crossref PubMed Google Scholar
2. Dattani R , Morgan C , Li L , Bennett-Brown K , Wharton RMH . The impact of COVID-19 on the future of orthopaedic training in the UK . Acta Orthop . 2020 : 1 – 6 . Crossref PubMed Google Scholar
3. An TW , Henry JK , Igboechi O , et al. How are orthopaedic surgery residencies responding to the COVID-19 pandemic? an assessment of resident experiences in cities of major virus outbreak . J Am Acad Orthop Surg . 2020 ; 28 ( 15 ): e679 – e85 . Crossref PubMed Google Scholar
4. JCST . Certification guidelines and checklists . 2018 . https://www.jcst.org/quality-assurance/certification-guidelines-and-checklists/ (date last accessed 30 September 2020 ). Google Scholar
5. Chang D-G , Park J-B , Baek GH , et al. The impact of COVID-19 pandemic on orthopaedic resident education: a nationwide survey study in South Korea . Int Orthop . 2020 . Crossref PubMed Google Scholar
6. Khan H , Williamson M , Trompeter A . The impact of the COVID-19 pandemic on orthopaedic services and training in the UK . Eur J Orthop Surg Traumatol . 2020 ; 368 ( 9 ). Crossref PubMed Google Scholar
7. Megaloikonomos PD , Thaler M , Igoumenou VG , et al. Impact of the COVID-19 pandemic on orthopaedic and trauma surgery training in Europe . Int Orthop . 2020 ; 44 ( 9 ): 1611 – 1619 . Crossref PubMed Google Scholar
8. JCST . Surgery specific management of ARCPs during COVID-19 . 2020 . https://www.jcst.org/key-documents/ (date last accessed 30 September 2020 ). Google Scholar
9. Schwarzkopf R , Maher NA , Slover JD , Strauss EJ , Bosco JA , Zuckerman JD . The response of an orthopedic department and specialty Hospital at the epicenter of a pandemic: the NYU Langone health experience . J Arthroplasty . 2020 ; 35 ( 7S ): S3 – S5 . Crossref PubMed Google Scholar
10. Stambough JB , Curtin BM , Gililland JM , et al. The past, present, and future of orthopedic education: lessons learned from the COVID-19 pandemic . J Arthroplasty . 2020 ; 35 ( 7S ): S60 – S64 . Crossref PubMed Google Scholar
11. Plancher KD , Shanmugam JP , Petterson SC . The changing face of orthopaedic education: searching for the new reality after COVID-19 . Arthrosc Sports Med Rehabil . 2020 ; 2 ( 4 ): e295 – e298 . Crossref PubMed Google Scholar
12. Siddiqi A , Chen AF , Schwarzkopf R , Springer BD , Krebs VE , Piuzzi NS . Evaluating the fellowship experience during COVID-19: adult joint reconstruction . J Arthroplasty . 2020 ; 35 ( 8 ): 1959 – 1961 . Crossref PubMed Google Scholar
13. Wilson JM , Schwartz AM , Farley KX , Devito DP , Fletcher ND . Doing our part to conserve resources: determining whether all personal protective equipment is mandatory for closed reduction and percutaneous pinning of supracondylar humeral fractures . J Bone Joint Surg Am . 2020 ; 102 ( 13 ): e66 . Crossref PubMed Google Scholar
14. Kadhum M , Farrell S , Hussain R , Molodynski A . Mental wellbeing and burnout in surgical trainees: implications for the post-COVID-19 era . Br J Surg . 2020 ; 107 ( 8 ): e264 . Crossref PubMed Google Scholar
Author contributions
G. A. Sheridan: Collected and analyzed the data, Reviewed the statistics, Wrote the manuscript.
A. J. Hughes: Collected and analyzed the data.
J. F. Quinlan: Designed the study, Edited the manuscript.
E. Sheehan: Designed the study, Edited the manuscript.
J. M. O'Byrne: Designed the study, Edited the manuscript.
Funding statement
No benefits in any form have been received or will be received from a commercial party related directly or indirectly to the subject of this article.
© 2020 Author(s) et al. This is an open-access article distributed under the terms of the Creative Commons Attributions licence (CC-BY-NC-ND), which permits unrestricted use, distribution, and reproduction in any medium, but not for commercial gain, provided the original author and source are credited. See https://creativecommons.org/licenses/by-nc-nd/4.0/.
